Equine tendons and ligaments
Tendon and ligament anatomy
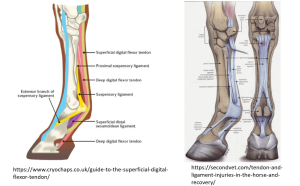
The key structures on the flexor surface of the cannon bone are the superficial digital flexor tendon, the deep digital flexor tendon, the inferior check ligament and the suspensory ligament. The structures change slightly in appearance and structure as you move distally from the carpus or hock. The structures combine to support the fetlock against the horse’s body weight. These are supported by the distal digital annular ligament, digital flexor tendon sheath and the distal sesamoidean ligaments.
Superficial digital flexor tendon
This is the most superficial structure, connecting the superficial digital flexor muscle to the second pastern bone (P2). The SDF tendon flexes the pastern and fetlock joints. It can be readily lacerated and is also affected by strain injury (tendonitis, bowed tendon). It is “checked” (restricted in motion) by the superior check ligament located above the forelimb carpus. (The hindlimb check ligament is vestigial.) If the SDF tendon is relatively too tight, it creates fetlock contracture.
Deep digital flexor tendon
The deep digital flexor tendon is the next most superficial structure. It extends from the deep digital flexor muscle to the bottom of the foot. This is the only flexor tendon that inserts on P3. Because of this very long path, the lower portion of the DDF tendon runs in a tendon sheath. The fluid in this sheath lubricates the tendon and helps it glide over the bony structures (including the navicular bone). The DDF tendon flexes the coffin, pastern and fetlock joints.
This tendon undergoes a lot of wear and tear as it passes over the navicular bone. It can become inflamed and can adhere to the navicular bone. Because of the restrictions from the adhesions, one consequence is rupture of the tendon. The tendon can also be lacerated with deeper injury. Rupture or complete laceration will typically result in a “toe up” stance on weight bearing. This tendon is also held in “check”; the inferior check ligament connects the DDF tendon to the back of the cannon bone. If the tendon is too tight, it results in a “club foot” or contracted distal interphalangeal joint. This deformity can be treated with transection of the check ligament as described below.
Inferior check ligament
The inferior or distal check ligament can be visualized ultrasonographically in the proximal third of the cannon bone. It is located deep to the deep flexor tendon and connects the DDFT to the palmar surface of the cannon bone. The check ligament “checks” the action of the DDF tendon+ muscle unit. When the check ligament is cut, the DDF tendon+muscle unit can stretch, releasing tension on the coffin joint. This surgery is used to realign the hoof-pastern axis contracture related to conformation and laminitis. The forelimb check ligament is of similar size to the DDF tendon; it is more vestigial in the hindlimb.
Suspensory ligament
The suspensory ligament is the deepest structure on the flexor surface of the cannon bone and extends from the proximal cannon bone to the sesamoid bones. It begins as a single structure (“body”) and then splits into two parts (“branches”). As a ligament, it resists stretch and maintains tension on the fetlock joint. If the suspensory is damaged, the fetlock can drop significantly. Damage to a ligament is referred to as “desmitis“. Limited blood flow and important structural roles mean ligaments heal slowly.
Distal sesamoidean ligaments
The suspensory ligament mainly attaches on the abaxial parts of the sesamoid bones and will pull up on them. Therefore, the distal sesamoidean ligaments are needed to pull “down” (distal) on the sesamoid bones. The 2 main distal sesamoidean ligaments are:
- straight = superficial ->short pastern bone (P2) proximal end between insertions of SDFT
- oblique = middle ->triangular area on palmar surface of long pastern bone (P1)
The sesamoid bones are bound to the distal end of the cannon bone by collateral sesamoidean ligaments. Sesamoid fractures are caused by the upward and downward pull on the sesamoid bones may cause them to fracture (fx) as in a “tug of war”. Sesamoid fx can be basal, apical or sagittal.
Intersesamoidean ligament
A fibrocartilagenous intersesamoidean ligament binds the sesamoid bones together so that the proximal sesamoids form a groove for the flexor tendons. The flexor tendons are held in this groove by the palmar annular ligament.
Palmar annular ligaments (proximal and distal)
The palmar annular ligaments bind the flexor structures to the limb by wrapping them tightly to the fetlock and pastern. This helps support the structures but it can also cause additional damage. When structures underneath the annular ligament try to swell (tendonitis, tenosynovitis), they can’t. This creates a compartment syndrome wherein the pressure created by the closed system results in additional damage. The annular ligament can also be damaged and thickened, creating a similar situation. When the annular ligament is too tight, the fluid in the tendon sheath will be seen to create bulges proximally and distally to the ligament. The annular ligament may need to be cut to release the pressure. See the description in the Tendonitis and desmitis chapter.
