Equine tendons and ligaments
How to – Inferior check desmotomy
Indications
Inferior check desmotomy is performed to treat contracture of the deep digital flexor tendon, particularly in the young horse. It may provide a window of security for Cushingoid horses with chronic laminitis and at risk of further rotation.
Relevant anatomy

The check ligament is between the body of the suspensory and the deep flexor tendon in the proximal cannon bone area. The distal or inferior check ligament connects the deep flexor tendon to the fascia on the palmar aspect of MC III. The diameter of the inferior check ligament is very similar to that of the deep and the two structures are merged together grossly. The line of separation is often better identified via palpation than by visualization. Ultrasonographic guidance is useful, particularly in standing surgeries. A large vessel runs along the medial aspect and can be accidentally cut during the surgery.
The check ligament in the hindlimb is vestigial and not usually a problem.
Preoperative management
Food restrictions: If the surgery is performed under general anesthesia, food should be restricted if possible (2-6 hours)
NSAIDs/analgesics: NSAIDs should be administered preoperatively and postoperatively.
Antibiotics: Not indicated
Tetanus prophylaxis is recommended.
Local blocks: Due to the location of the incision, any local block would need to be performed above the carpus (MUM block).
Position/preparation:
Clip from above the carpus to the distal cannon bone on a foreleg. The lateral approach is the easiest (and avoids that very large vessel that tends to be directly in your way). Wrap the foot in a sterile towel to enable manipulation of the toe.
The procedure is done under general anesthesia in young animals but may be done standing is select patients with ultrasound guidance.
Surgery Supplies:
- Drapes or sterile towels
- Scalpel blade and handle
- Hemostatic forceps (curved and straight)
- Bistoury
- Needle holders
- Suture- 3-0 absorbable taper needle
- Suture – 3-0 absorbable cutting needle
- Suture – 3-0 nonabsorbable
- Bandage supplies
Surgical procedure
A 3-cm skin incision is made over the cranial aspect of the deep digital flexor tendon approximately 3-cm distal to the carpus (center over junction of proximal and middle thirds) The incision is continued through the fascia and peritenon (covering over the tendons). The deep digital flexor tendon and the check ligament are isolated by blunt dissection. These at first appear to be one large tendon but there is a plane separating them. The check ligament is about the same size as the deep digital flexor tendon!
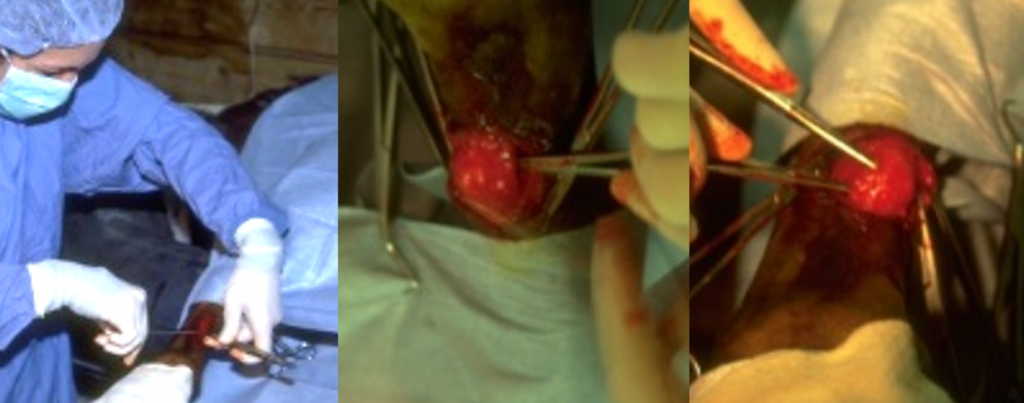
Move the toe to see how much tension is on the structures. Once identified a mosquito hemostat is used to bluntly separate the check ligament from the DDF. A second hemostat is then placed between the suspensory ligament and the check ligament. By then turning the points of the hemostats together the check ligament is isolated. Once isolated, the check ligament is sharply transected using a scalpel or bistoury knife. If you are unsure if you have three separate structures, suture material can be passed around the “check ligament” and then the ligament returned to the incision to allow better inspection. The check ligament should gap if all fibers are cut particularly when the toe is extended. The peritenon and fascia are closed with a simple continuous pattern. The skin is closed routinely, often with an intradermal pattern.
Postoperative care
- The incision is covered with gauze and a support bandage applied to the limb.
- To ensure that the ligament does not scar in the original position, farrier work and physical therapy are essential. The foot should be trimmed to a normal angle (lowered heel) and the animal treated with NSAIDs or other analgesics to encourage use of the limb. If the foal cannot tolerate NSAIDs, fentanyl patches are an alternative.
Complications
- incomplete transection of the ligament
- damage to the medial vessel
- damage to the deep flexor tendon and/or suspensory ligament
- limited response due to lack of farrier work and exercise
Videos
Resources
Flexural deformity of the distal interphalangeal joint, VCNA 33(2):315-330
cutting of a ligament
tightening of the tendons leading to a bowing effect of the limb
