Equine Colic
Gas and impaction colics
The majority (80%) of colics are gas or impaction colics. They look very similar. They are treated very similarly and respond well to field treatment. Both have a good prognosis as long as the causative factors are managed.
Impaction colics
The majority of impactions are pelvic flexure impactions and may develop for 3 main reasons:
- Foodstuffs are not easily digestible. Ex: Poor mastication due to speedy eating, poor dentition, or poor quality feeds
- The gut isn’t able to digest things well due to a change in motility or change in flora activity. Ex: atropine treatment for eye issues, pain or illness, exercise changes, feed changes. Sand weighs down the guts and hinders motility as well as eroding the mucosal lining.
- The ingesta doesn’t slide well due anatomical and physiological challenges (there are lots of these) or because the ingesta is dry, hard or sticky. Ex: dehydration, enterolith formation
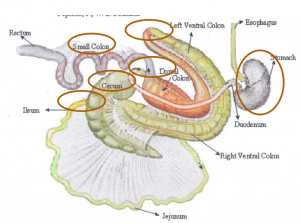
Anatomical and physiological challenges
- Friesians have abnormal gastric motility
- Ileal break reflex slows emptying
- Pelvic flexure creates a hairpin turn with narrowing
- Cecum is blind-ended
- Small colon is narrowed
- Absorption of water from the small colon
Gas colics
Gas or tympanic colics develop when:
- Diet changes result in increased gas production by the microbial flora. Ex: diets high in corn (fermentable), sudden feed changes
- Motility changes prevent farting and/or result in more fermentation due to delayed transit times. Ex: pain, atropine, electrolyte abnormalities (endurance racing, hot weather).
Diagnostics
- Both gas and impaction colics lead to mild to moderate colic signs and decreased manure production. Heart rate is generally only mildly elevated (40-60bpm). Horses can become mildly dehydrated. Horses may look bloated with gas colics. Reflux is not generally seen.
- Differentiating between gas and impaction colics requires rectal palpation and even that may be inconclusive. However, both can be managed similarly so the challenge is only in differentiating field vs referral colics.
Treatment
Rehydrate/overhydrate
- Give fluids orally via nasogastric tube and/or iv. Oral is more effective! Generally give 4-8L (or 1 to 2 gal) total to 1000# horse.
- Gastric distension stimulates colonic activity through the gastrocolic reflex
- If you have difficulty passing the nasogastric tube into stomach due to esophageal sphincter tone, infuse 25-30 ml lidocaine via the tube
Provide pain relief
- Pain stimulates the flight response and shuts down motility
- NSAIDs such as flunixin meglumine are commonly used (remember – don’t give banamine im due to the risk of clostridial myositis)
- Buscopan (gut muscle relaxant) can be given once to help with intestinal spasms. This helps gas colics more than it helps impaction colics. Note : it will cause an elevated heart rate for 30 minutes!
Stimulate motility
- Walk horses to stimulate GI motility
- Grazing may also help (grass, not hay)
Prevent worsening
- Remove hay and grain (grazing grass is okay) until the horse poops
Consider laxatives
- Magnesium sulfate (Epsom salts) are the primary laxative used to treat feed impactions. Horses should not be given more then 1g/kg/day (about 1 pound per day in 1000lb horse). This is administered orally via the NG tube in 4-6L of water. CAUTION: Horses with gastric ulcers can become very colicky after administration (as you can imagine, OUCH!) and indicates referral for gastroscopy.
- Dioctyl Sodium Sulfosuccinate (DSS) is a laxative but rarely used in the USA due to the potential of inducing a severe colitis.
- For a feed impaction, mineral oil can be used to help determine transit time but is really ineffective at breaking up the impaction. Mineral oil can help with gas colics as it breaks up some forms of bubbles.
- If sand : psyllium 0.5 g/kg PO BID or 1g/kg PO SID combined with the same dose of magnesium sulfate or with 2L mineral oil. Psyllium is the main ingredient in metamucil; it is a soluble fiber that is hard to digest and pulls water into the manure. Magnesium sulfate is also an osmotic laxative has been shown more effective than mineral oil. The concoction can be given in place of oral water via nasogastric tube. You can read more about sand impactions in the impactions chapter.
Monitor response to treatment
- Signs of pain continue
- Horse defecates
- Perform rectal palpation if indicated and safe to determine if the impaction is resolving
- Most impaction and gas colics will resolve with just one visit. Refer if severe, not manageable, or not responding within 12-24h! That typically means they are in the other 20% of colic types.
- Young horses with perirectal abscesses can develop secondary rectal impactions and gas colics. These are rare and are associated with tenesmus, dyschezia, and abdominal distension. In most cases, the mass is palpable per rectum. Transrectal ultrasound examination is very helpful in identifying signs consistent with abscessation.
Resources
- Management of colic in field, 2021 VCNA
- Diagnosis and management of sand enteropathy in the horse, 2022 EVE
- Diagnosis, management and prognosis of large colon impactions, 2021 EVE
- Caecal impactions: Diagnosis, management and prognosis, 2021 EVE
- Facts and myths about medical treatment of colic, 2017 FAEP
- Colic due to dorsally located perirectal abscesses, 2023 EVE
definition
blockage or partial blockage of the intestinal lumen by feedstuff
