Food/Fiber Cesarean Sections
How to – Left Flank Csection
Indications
Cesarean section is indicated for many causes of dystocia, as a preventive measure for animals with anticipated dystocia and for gnotobiotic calves.
Relevant anatomy
The uterus can be accessed from either side. The rumen holds in the intestines on the left, making that the preferred approach. The uterus can be challenging to exteriorize via the left flank if the pregnancy is in the right horn or with uterine torsions. A ventrolateral approach is preferred for weak cows, damaged or emphysematous uteri.
The body of the calf will be in the pregnant horn, forcing limbs into the nonpregnant horn. That makes the nonpregnant horn easier to manipulate.
Preoperative management
Food restrictions: NA
NSAIDs/analgesics: Recommended preoperatively. Flunixin meglumine 1.1-2.2 mg/kg iv is standard.
Antibiotics: Recommended if any vaginal manipulation or prolonged dystocia. In general, the cervix is open and preoperative manipulations ensure the uterine fluids are contaminated. Timing is important to ensure the drugs are at high concentrations at the time of surgery (see earlier chapter). If milking, ceftiofur 2.2 mg/kg im is standard. In beef or non-lactating cattle, other options do exist. Remember: the label dose of procaine penicillin is ineffective!
Local blocks: A line block, inverted L or paravertebral are all reasonable options. A line or inverted L is required for an oblique incision as the paravertebral will not cover the ventral aspect. An epidural can help minimize straining if the cow is actively in labor.
Sedatives: Local blocks are often sufficient. If more sedation is required, just try to avoid xylazine. I prefer acepromazine/butorphanol combinations. Detomidine does not cause uterine contractions and is another option; it can also be used with butorphanol.
Epinephrine relaxes uterus? 10ml 1:1000 diluted iv preop
Position/preparation: See How to- Standing GI Surgery
Position/preparation: Standing. Healthy cows tolerate standing surgery very well. Many do not need sedation but will do fine with just a local block. However, if they are heavily pregnant, (and particularly if they are Jerseys) they may just decide to lie down in the middle of the procedure. If this is a concern, we try to make it more likely that she will land incision side up.
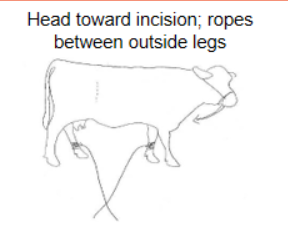 Place ropes on the far legs and tie her head toward the incision. If she starts to lie down, nonsurgical personnel pull on the ropes and pull her legs out from under her. With the head tied in this direction, she is also more likely to fold that way and stay incision side up.
Place ropes on the far legs and tie her head toward the incision. If she starts to lie down, nonsurgical personnel pull on the ropes and pull her legs out from under her. With the head tied in this direction, she is also more likely to fold that way and stay incision side up.
An assistant is almost always necessary. This can be an untrained assistant that is garbed in sterile gloves (rectal sleeves are fine) and told what to touch and not touch. If the calf is alive, another person is needed for calf care and should be asked to set up an area for drying and warming the calf. This person can act as a nonsterile assistant and help with calf removal etc.
Surgery Supplies – Supplemental
- 2 absorbable suture material for uterine closure
- Calf hooks and chains
- Oxytocin
- Uterine forceps – optional
- Sterile envelope cutter – optional for incising the uterus
- Gigli wire and handles – optional
Surgery Supplies – Standard
- Standard surgery pack
- Sterile sleeves for internal palpation
- Scalpel blade and handle
- 2 or 3 absorbable suture material for muscle closure
- 3+ nonabsorbable suture material for skin closure
Surgical procedure
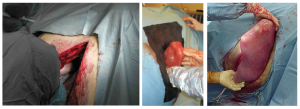
After the cow is clipped and prepped, a 40 cm vertical or 40-50 cm oblique incision in made starting in the caudal third of the paralumbar fossa and continued through all muscle layers and the peritoneal cavity. The flank incision should be just long enough to exteriorize the calf’s hindlimb from toe to point of hock. An incision smaller than this will prevent calf removal; a larger incision much longer will make it hard to hold the calf out during the Csection.

Once the cavity is open, sterile sleeves and overgloves (surgery gloves that are a size bigger) are placed on both arms. Instruments for closure should be separated and covered to keep them clean.
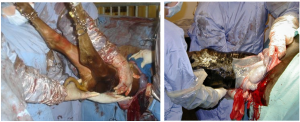
The uterus and any torsions are identified. If the calf is in typical position, a hindlimb is grasped and brought to the incision (forelimb if the calf is breech). With careful rocking and manipulation, the nonpregnant horn containing the hindlimbs is brought to the incision. The healthy uterus can tolerate a fair bit of force but whole hand manipulation should be used rather than fingers which can cause more damage. If the pregnancy is in the far (right) horn, the surgeon reaches underneath, grasps the top of the uterus and pushes it down and pulls it over to the left side, creating a 180 degree torsion.
Once the hindlimb is identified, it is grasped and brought out the incision. If the limb can be hooked out the incision, that helps prevent the calf from moving away again.
At this stage it is important to ensure everyone knows the plan.
Someone must keep the uterus held out so that the uterine contents drain outside of the cow. [The uterine contents are considered contaminated due to the vaginal manipulations in most dystocias.] The sterile assistant is generally given this job. A moist hand towel or padded uterine forceps can be used to maintain a grip on the uterus at the top and bottom. Holding in the middle means being in the way of the scalpel blade during the Csection. It is tempting to let go once the calf is out; it is important that this person stay holding the uterus. The job is hard until the calf is removed.

- Chains are applied to the paired limbs (both forelimbs or both hindlimbs). See this video for how to apply chains to avoid damage. Apply triangle hooks to help hold the chains (apply hooks as close to the calf as possible for best leverage and lift).
- Someone will take the chain hooks/chains and pull the calf out. This person can be nonsterile. The calf will need to be pulled upwards first and then horizontally. A taller person can be helpful (or a stepstool). This person must follow the surgeon’s direction on when to pull.
- Someone to create the incision in the uterus; typically the surgeon. The surgeon will also manage the rest of the team, directing when to start and stop pulling.
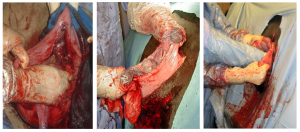
The incision is made between caruncles (to avoid bleeding) starting at the tip of the toes. The eponychium will protect the calf from damage if the scalpel goes a little too deep. Either a scalpel or envelope cutter can be used. The amnion is incised.

Once the foot is accessible, chains can be put on the limb to prevent the calf from moving away. A double loop is recommended to avoid too much pressure in one site. The chain is passed off to the nonsterile assistant to grab with a hook. No pulling is needed yet, just holding.

The incision can then be lengthened sufficiently to find the other matching foot. Another chain (or other end of a long chain) is placed on this foot and handed off as before.

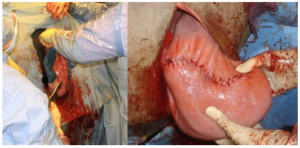
At this stage the uterus is firmly grasped by the sterile assistant and the incision in the uterus lengthened to the point of the hock. If the incision is not long enough, the uterus will tear. The surgeon can and should stop the action at any point if it is deemed a longer incision is needed.

The calf is pulled out (upwards and then horizontally) as it is supported by the surgeon. The umbilicus should tear naturally. If not, the cord is held at each end and torn by pulling the ends apart. The calf can be taken to the prepared area.
The amnion can be pulled off or pushed into the uterus. Any fluid can be dumped on the ground outside of the cow. The surgeon should check for any other calves or uterine tears.
The uterus is closed in two layers. One layer is often described in the literature but that suture line becomes loose as the uterus contracts, making a second advisable. Any inverting pattern can be used (Lembert, Utrecht, Cushing). Absorbable #2 with a swedged on needle is advised. Full thickness patterns are not recommended and appositional and everting patterns can lead to adhesions. The placenta is not usually ready to be removed so should be pushed into the uterus. Care should be taken to avoid suturing the placenta into the incision line.
Once the first layer is completed, the sterile assistant can relax. Blood clots are removed from the uterine surface and a second layer of closure performed. The cow should be given oxytocin after the first layer is closed to ensure good involution (and a tighter suture line) during the second. The uterus is returned to the abdominal cavity and checked once again to ensure normal position, no other calf and no tears.
Closure : Follow the guidelines for standing GI surgery.
Postoperative care
- NSAIDs and antibiotics should be continued for at least three days if any risk of uterus contamination
- Oxytocin (10-40IU im) helps with uterine contraction but does not help with retained placentas.
- The placenta is tied in a knot to add traction but is left to pass on its own
Complications
Almost all cattle will develop retained placentas. There is recent evidence that flunixin meglumine increases this risk. However, NSAIDs do a lot of good things and retained placenta is readily treated in cattle. These are not as life threatening as in horses and managed with oxytocin and time.
Incisional infections may develop and are treated by removal of a distal suture to allow drainage
Videos
Youtube video– great James Herriot type video of a heifer Csection. Lots of advanced technology and hilarious
Video 1– opening peritoneum
Video 2 – exteriorizing calf
Video 3– incising uterus and exteriorizing limb
Video 4 – pulling calf
Video 5 – prep for closure
Video 6 – closing uterus and burying knot
Resources
suture pattern in which tissue edges are turned inward
suture pattern in which the cut edges are turned outward
