Equine joint disorders
Hock joint problems
Older horses get arthritis; osteochondrosis is more likely to be diagnosed in a young horse.
Anatomy
The tarsal joint is really a collection of four joints, some of which communicate with each other but there are horse to horse differences.
Tarsocrural = tibiotarsal joint
This is the big joint and is where all movement occurs. It always communicates with proximal intertarsal joint. Effusion of this joint is known as bog spavin.
To tap or inject this joint : Inject slightly distal to medial malleolus and more dorsal so the needle does not pass thru the medial collateral ligaments which come off the distal end of the medial maleolus. Needle should pass into the large joint space between the medial collateral ligament and the cranial branch of the medial saphenous vein.
Proximal intertarsal joint
This is a low motion joint between the talus/calcaneus and the central tarsal bone + T4. This joint always communicates with the tibiotarsal joint so separate injection is unnecessary. Inflammatory mediators within this joint will also affect the tibiotarsal joint.
Distal intertarsal joint
This is a low motion joint. Arthritis in this joint is called bone spavin.
Injection of the distal intertarsal joint is the most difficult due to narrow space and heavy covering with the medial collateral ligaments. An imaginary line is found between the distal (medial) tubercle of the talus and the groove between medial splint and the cannon bone. The injection point is on this line and just distal or thru the cunean tendon distal edge. The goal is to pass the needle tip into the intersection of Tc with T3 and T1+2.
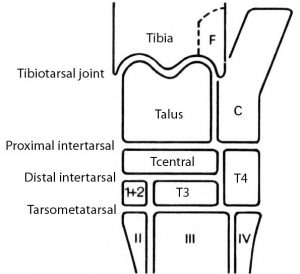
Tarsometatarsal joint
This is a low motion joint. Arthritis in this joint is also called bone spavin. In 10-40% of hocks this joint will communicate with the distal intertarsal joint. Some drugs may also diffuse across these joints.
To inject this joint, pass the needle tip on the lateral side between T4 and edge of the head of lateral splint (Mt 4).
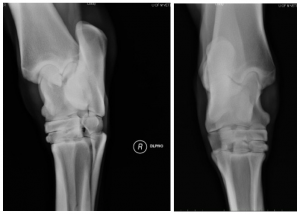
Normal radiographic anatomy
The tarsal joint has more complex ligaments than other joints. It has long and short collateral ligaments. Long collateral ligaments extend from the tibia to the metatarsus and are superficial to the short collateral ligaments. Short collateral ligaments extend from the tibia to the talus or calaneus or both. Superficial, middle and deep short collateral ligaments have been described. Additionally there is a large dorsal tarsal ligament running from the distal (medial) tubercle of the talus to the cannon bone (Mt3), Tc and T3. The long plantar ligament runs from the plantar aspect of the calaneus to the head of the lateral splint bone (Mt 4). It is torn in curb. Other ligaments bind together individual tarsal bones.
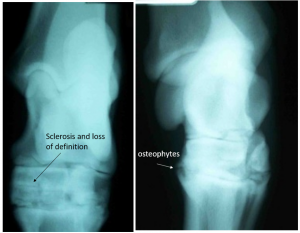
Osteoarthritis
Bone spavin is arthritis of the distal hock joints (tarsometatarsal and distal intertarsal joints). These are low motion joints but are affected by normal wear and tear due to gliding, stopping, and turning. Most older horses that have been in any degree of work will have changes in these joints. Some younger horses may also have changes, despite not being in work. The changes in younger horses are suspected of being due to cartilage abnormalities (form of osteochondrosis).
Hock joint arthritis is common in many performance horses.
- Standardbreds (harness horses): while a rider will shift the center of gravity towards the forelimbs, a rider in a sulky (cart) will shift the center of gravity towards the hind limbs and thereby increase stress on the tarsal joints.
- Rodeo horses that turn quickly stress their tarsal joints with rotary motion under a load.
- Jumpers stress their tarsal joints when they rear up and then propel themselves with their hind limbs. Poor conformation as in “cow hocked” individuals is another contributing factor
Diagnosis
Horses with bone spavin will have an abnormal gait with a low foot flight because tarsal flexion is painful. Upper limb flexion will make the lameness worse.
Relief of pain after anesthetic injection of the cunean bursa or distal intertarsal joints. The injection sites are as follows:
- Distal intertarsal – at T-shaped junction of Tc, T3 and T1+2
- Tarsometatarsal – at junction of T3, T4 and Mt3. Remember that the collateral ligaments cover over the joints and make injection difficult.
Radiographic lesions include osteophytes (new bone at the edges of joints) which make the bone edges sharp or appear to have spikes, loss of joint definition (lack of a sharp line) due to cartilage loss and bone formation in the space, and mild remodeling of the boney shapes – the joint may look fuzzy.
Therapy
Because these are low motion joints, treatment is aimed at fusing the joints so that motion (and therefore pain) no longer occur. This can be done by keeping the horse in work (and on analgesics); however, it may take some time for natural fusion to occur. The process can be speeded by injecting the lower joints with steroids, injecting them with a compound that destroys cartilage (monoiodoacetate or MIA; no longer in favor), or by removing the cartilage with a drill while the horse is anesthetized. Historically, cunean tendinectomy was performed to relieve pressure on the remodeled bone. Prognosis is favorable as long as only the lower two joints are affected. Since the proximal intertarsal joint communicates with the high motion tibiotarsal joint, changes in that joint are more serious and can lead to arthritis in the tibiotarsal joint.
Recent work by Coomer et al suggests stem cell injections may be useful for tarsometatarsal pain.
More details about therapeutic options in the Osteoarthritis chapter.
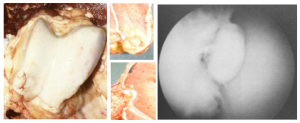
Osteochondrosis
Osteochondrosis dissecans is a developmental disorder whereby pieces of cartilage +/- bone break off.
Clinical signs include joint effusion with minimal lameness. Young horses just being put into work are most commonly affected.

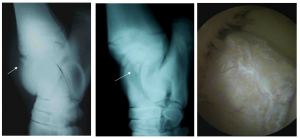
The predominant sites in the hock are the distal intermediate ridge of the tibia (known as DIRT lesions) and the lateral trochlear ridge of the talus. The medial malleolus can also be affected.
OCD is often a bilateral condition so both hocks should be radiographed. Fragments of bone may be apparent in the joint. Arthroscopic surgery may be necessary to find cartilage fragments and is the treatment of choice. Once the fragments are removed, horses with hock OCD have a very good prognosis for future performance.
More details about therapeutic options in the Osteochondrosis chapter.
Capped hocks

Capped hocks are due to bursitis and are generally related to trauma. Note the swelling is more localized to the point of the hock.
Other lesions include infections, fractures of the cuboidal bones and hock luxations.
Key Takeaways
Young horses get joint effusion from osteochondrosis. The most common site is the tibiotarsal joint with a fragment off the distal intermediate ridge (DIRT lesion)
Older horses are painful due to arthritis. Arthritis most typically affects the lower joints: tarsometatarsal and distal intertarsal joints. This is referred to as bone spavin.
Resources
Anatomy and radiography of the equine tarsus ibook
Review of equine distal hock inflammation and arthritis, AAEP 2006
Diagnosing lameness in the tarsus and proximal suspensory region, FAEP 2017
Osteochondral fragments from the
Distal
Intermediate
Ridge of the
Tibia
