Swine, SRC and poultry lameness
How to – Forelimb amputation
Indications
Limb amputation is recommended when the limb is painful and unlikely to improve, vascular supply is damaged, deep structures are infected, or when orthopedic stabilization is not possible (comminuted fractures, etc). In most cases, prostheses are not used. This description is for management of the animal when a prosthetic limb is not planned. Forelimbs may also be amputated by disarticulation of the scapulohumeral joint.
Relevant anatomy
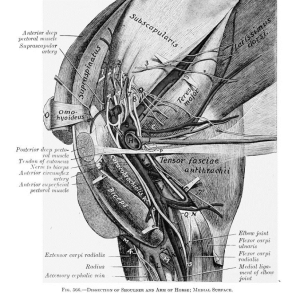
The entire forelimb is removed with this approach. Dissection involves removing the scapula by cutting its muscular attachments to the torso, transecting the nerves and ligating the major vessels.
Preoperative management
Food restrictions:
The procedure is performed under general anesthesia. Food should be withheld for 48 hours whenever possible.
NSAIDs/analgesics: Preoperative and postoperative analgesics are recommended.
Antibiotics: Not usually required.
Local blocks: Could consider a brachial plexus block; can also inject or infused lidocaine when nerve is exposed
Position/preparation:
The animal is positioned in lateral recumbency with the limb suspended. The entire limb should be draped. The vertical limb permits access from all directions and the complete draping allows for full manipulation.
Surgery Supplies:
- Standard surgery pack
- 2-0 absorbable suture, taper needle
- 2-0 nonabsorbable suture, cutting needle
Surgical procedure
- Using the scalpel blade, make an inverted Y shaped incision. The base of the Y should follow the the spine of the scapula to the greater tubercule. One branch of the Y extends from the greater tubercle halfway to the elbow. The other branch extends from the greater tubercle to the fold of the axilla
- Major veins and major arteries are double ligated with 2-0 absorbable suture. These vessels should be ligated separated to avoid the formation of an arteriovenous fistula.
- Muscles are trimmed away from the scapula and humerus close to the bone, leaving more muscle to cover the body. When possible, transect through a tendon of insertion ot minimize hemorrhage. As muscles are cut, hemostasis should be managed with electrocautery or ligation.
- Nerves are pulled gently distally and then severed. The nerve ends are allowed to retract naturally. Extension traction or crushing should be avoided.
- The forelimb vasculature should be ligated proximal to the greater tubercle.
- After the superficial muscles are cut, the cranial edge of the scapula is rotated externally to allow transection of the rhomboideus and serratus ventralis muscles. The suprascapular artery, vein and nerve are transected with the vessels being double ligated.
- The pectoral muscles are then transected at their attachment to the humerus.
- The subscapular nerve and brachial plexus are transected. The axillary artery is double ligated and transected as is the axillary vein.
- The limb is now separated and removed from the surgery table
- The cut ends of the muscles are turned inwards. The lateral fascial sheaths of the latissimus dorsi, omotransversarius and trapezius muscles are sutured to the lateral fascial sheaths of the pectoral muscles. Absorbable sutures in a mattress pattern or continuous pattern are used.
- Drains may be placed in dead space
- Trim excessive skin if needed. Avoid both excessive tension and excessive skin.
- Suture the skin using 2-0 nonabsorbable suture, avoiding having the incision run directly over pressure points such as the acromion. Start by apposing the skin flaps with interrupted sutures. The remaining closure can be performed using any appositional skin suturing pattern.
- Apply an elastic compression bandage to minimize edema and eliminate dead space.
Postoperative care
- The bandage is typically changed daily for 3-5 days.
- Assist the patient with standing and walking until they are able to do so without placing pressure on the amputation site
Complications
- hemorrhage
- minor hemorrhage can be controlled by a pressure bandage; more substantial hemorrhage will require repeat anesthesia/surgery and ligation of the bleeding vessel
- infections
- treat with hot packs and drainage
- skin ulceration
- treat with hot packs, excision of ulcerated tissue, and wound closure without tension
Videos
Forelimb amputation in a dog -video link
Resources
Clinician’s brief forelimb amputation – 2013, Selm. Includes video
Amputation, Veterian Key
