Eye surgery
How to – Exenteration
Indications
Eyes may be removed due to trauma, infection, neoplasia or pain (ulcers, glaucoma, uveitis). Enucleation may be the quickest way to a comfortable animal and can decrease the risk of spread of tumors or aggressive infections.
Relevant anatomy
The optic nerve should be blocked with local anesthetic prior to surgery, even with animals under general anesthesia. The optic nerve can be accessed in a variety of methods. See Ocular blocks.
Cattle have a deep bony orbit; horses have a complete bony orbit as well but it is wider so easier to access caudal structures. The ocular artery and optic nerve are at the back of the globe in the center of the orbit. The remainder consists primarily of extraocular muscles and the third eyelid.
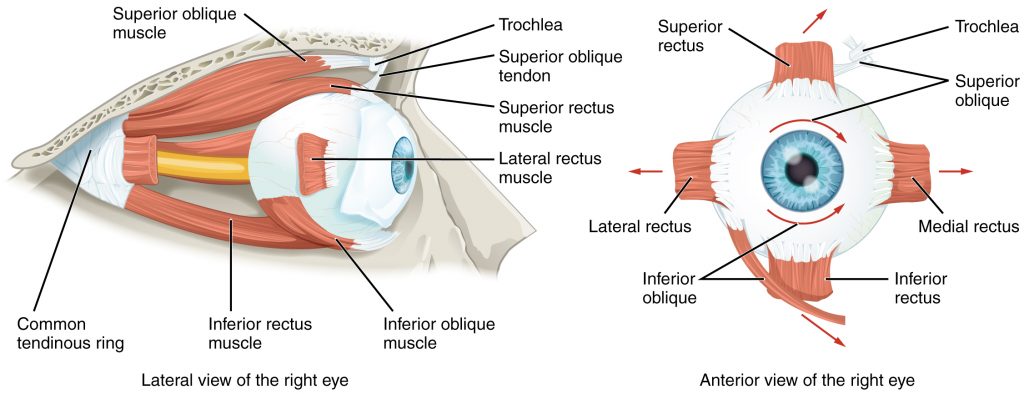
The third eyelid and it’s gland should be removed or the animal will continue to produce tears.
Preoperative management
Enucleation can be performed standing in many horses and cattle. This increases the safety by decreasing the likelihood of extensive hemorrhage and the risks of anesthesia and recovery. In small ruminants, sedation is typically needed. General anesthesia may be needed in some horses with extensive SCC to enable more cosmetic reconstruction.
Food restrictions:
NA unless general anesthesia is indicated.
NSAIDs/analgesics:
Preoperative and postoperative analgesics are required.
Antibiotics:
As the eye is not a sterile environment, preoperative and postoperative antibiotics are indicated. Broad spectrum coverage is indicated but first line drugs are fine (penicillin + gentamicin (equine), cephalosporin, ampicillin).
Tetanus prophylaxis is recommended.
Local blocks:
Options to block the ocular nerve include various forms of retrobulbar block including the Peterson nerve block. All are effective if performed correctly. If blocked, the pupil should dilate.
In my hands, the curved needle retrobulbar block is easy and effective
Position/preparation:

The animal is positioned in stocks or head gate (standing sedation) or in lateral recumbency with the affected eye uppermost. A head tray or dental halter can help hold the head still and at a reasonable level. The eye is clipped and prepped.
Surgery Supplies:
- Surgery pack
- Scalpel and handle
- Right angle hemostats (optional)
- Ecraseur (equine only )
- 2-0 or 0 suture on a cutting needle to close the lids
- 0 monofilament absorbable for the artery
- 0 suture on a cutting needle for the skin closure
Surgical procedure
The eyelids are sutured closed. The ends of the suture tags are left long as handles. Alternatively, towel clamps can be placed at each canthus. Towel clamps or allis tissue forceps are useful as they hold themselves closed; this is much easier on the surgeon as compared to holding tissue forceps closed.
A fusiform incision is made around the eyelids, pointy ends at the canthi, staying close to the lid margin. ** Incisions too far away from the lid margin can be challenging to close.**

Continue dissection through the retrobulbar tissues using mayo scissors (scalpel dissection may be needed at the canthi). Stay close to the bony orbit, going deeper rather than across the surface. Whenever possible, use scissors instead of a scalpel. The tissue trauma associated with scissors activates the clotting cascade and bleeding is lessened.
Work around the full circumference, moving deeper with each pass. Cut anything in your way. Digital palpation helps identify what needs to be cut.

If the dissection exposes the globe, ensure you also remove the third eyelid and gland. This will come out naturally if the globe is not exposed.
Once the only structures left are at the caudal aspect of the eye, prepare your suture for closure. Typically we do not clamp the artery in large animal species. In horses, an ecraseur can be used to crush and sever the artery. This does not work in cattle due to the anatomy of the orbit. In cattle, cut the artery with scissors.

Closure: Trim the eyelid margins and close the lids in a simple continuous pattern with 0 suture material. The needle on 2-0 suture material makes it difficult to be efficient.
Postoperative care
- Antibiotics are often continued for 5 days; NSAIDs are continued for 3 days.
- Monitor the incision for any signs of inflammation or infection. Sutures can be removed to allow drainage if necessary
- Prevent the animal from rubbing the area. Fly masks work well.
- Suture removal in 10-14 days
Complications
Contamination
If the incision should not be closed fully due to contamination and risk of infection (eg you would create an abscess), the socket can be packed with betadine soaked gauze and closed partially. The partial closure and packing will put enough pressure on the artery to create hemostasis. The packing can be removed gradually over the next few days.
Infection
Open the suture line partially or completely to allow drainage.
Incomplete closure
If the lids cannot be closed due to excess skin removal, the following options may help
- undermine and mesh the skin – make sure this area is over bone, not over the socket if hemorrhage is present
- remove brow bone – using an osteotome and mallet, this bone can be removed to create less of a bump
- leave it open – pack and cover with a stent bandage

Tumor recurrence
Owners should be counseled to watch for growths or ulceration that could indicate tumor recurrence.
Videos – these are graphic!
Resources
