Large animal wounds
Evaluation for factors that impair wound healing
Many factors can impede wound healing and make the after care challenging. Owners should be fully aware of the main risks and time line before starting on the journey.
Complicating non-urgent factors
Is the wound below the hock or carpus or involve eyelids?
- Distal limb wounds are prone to proud flesh
- Eyelid lacerations can lead to exposure keratitis if not managed appropriately
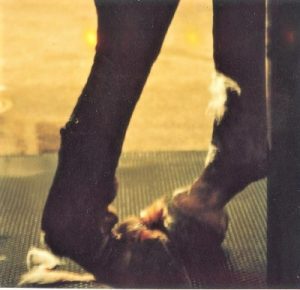
Is the horse knuckling over?
- Stabilization will be needed
Is there skin loss in a wound on the distal limb?
- Predisposed to proud flesh
Is bone exposed or damaged?
- Predisposed to sequestrum and/or infection
Is there muscle injury to the hindlimbs?
- At risk of fibrotic myopathy
Sharp or blunt trauma?
- Blunt trauma will lead to delayed damage
How heavily contaminated?
- Closure may not be recommended
Horse factors
- Will the horse allow treatment standing? tolerate bandage changes?
- Intended use and timeline for performance, if any?
- Adequate BCS and nutrition?
Chronicity
- How long has it been going on and has it been treated appropriately?
Wound location
Wounds below the hock and carpus are much more challenging to manage than wounds above the hock or carpus due to the risk of damage to deeper structures and to the risk of exuberant granulation tissue.

Wounds on the upper limb tend to heal well, even with muscle damage or skin loss. “Proud flesh” doesn’t happen above the carpus or hock for strange and mysterious reasons.

Wounds of the head tend to heal well due to the high vascularity of the head structures, including bone. However, wounds of the eyelids or periocular structures should be evaluated and managed carefully to identify and prevent globe damage from incomplete lids (exposure keratitis) or uneven lids (corneal ulcers from rubbing).
Extensor tendon damage
The extensor tendons run on on the dorsal aspects of the limbs and are important for limb position. The extensor tendon flips the foot forward so that it lands on the solar surface. When the extensor tendon is transected, the horse will tend to knuckle forward and be unable to flip the foot into the normal position. Once the limb is flipped forward, the horse can weight bear normally. These injuries heal quickly with little residual deficits. Suture repair of the tendon is not needed or warranted.
Skin flap or skin loss
Horse wounds often have missing skin or large skin flaps. Skin flaps will survive only if they have adequate blood supply. If the base of the flap is proximal (on the body side) it generally has good blood supply if it is wide enough. Flaps that have the base distal (on the foot side; away from the blood supply) often do not survive. Flaps with a thin base will often die off, as will the tip of triangular flaps. These flaps can be used to “bandage” the wound but will generally need to be debrided to permit complete wound healing.

Many wounds cannot be closed primarily. Horse limbs have very little loose skin to cover wounds and wound healing is often delayed or impaired by missing skin. Missing skin leads to wound dessication (drying) and potentially to bone sequestration. Wounds below the hock and carpus that are left open to heal often develop exuberant granulation tissue.
Periosteal or bone damage
Due to limited soft tissue covering, many injuries to the equine distal limb damage the periosteum and expose the bone. This can lead to sequestrum formation. Sequestra are pieces of dead bone that develop over 2-3 weeks and lead to persistent draining tracts.

Muscle injury
Muscle heals well and muscle injury does not usually complicate wound healing unless the resultant scar tissue is restrictive. This is a concern when the semitendinosus and semimembranosus muscles are damaged. Injuries in this area (caudal aspect of the hindlimb above the hock) can lead to fibrotic myopathy. Fibrotic myopathy is a gait abnormality in which the forward stride is restricted. As the limb moves forward, the muscles are designed to stretch to allow full arcing motion. However, if there is scar tissue in the muscles, they only stretch so far. The limb is then slapped down to the ground suddenly. The gait abnormality is most readily seen at a walk and is nonpainful.
Sharp or blunt trauma
Injuries with sharp objects (including incisions) are less traumatic than blunt trauma and ripping forces. With blunt trauma, the wound tissues continue to deteriorate over time. This may mean any initial repair falls apart. Swelling continues to increase over the first 3 days. Natural wound debridement is also occurring over this time period, sometimes leading to weaker tissue in the repair. If the wound is going to dehisce, that process usually starts between 2-3 days after wounding.

Clean or contaminated wound
Unless the wound occurs during surgery (eg an incision), most equine wounds are considered contaminated. Some are heavily contaminated with mud or manure from the start; others are minimally contaminated. As with other species, all wounds are considered to be infected after 6 hours (the golden period). Closure at this stage will often lead to abscess formation unless the wound is well debrided and/or ventral drainage is created.
Wounds entering the sinuses or airways are considered contaminated as are those entering the GI tract.
Wounds to the urogenital structures are considered contaminated. These wounds tend to swell significantly with the swelling leading to secondary issues such as preputial prolapse, paramphimosis and urinary obstruction. These tissues do have good healing potential but the healing process should be monitored to detect issues early.

Horse factors
Due to the risk of general anesthesia and recovery, horses are treated standing whenever possible. If the horse does not tolerate standing surgery, risks are increased. Similarly, some horses do not tolerate bandage changes. Depending on the wound, that can increase complication rates. Don’t forget to include your safety in the planning.
Horses that are underweight, parasitized or otherwise have low protein will have more difficulty with healing. Adequate nutrition and protein stores are necessary for wound healing.
Cushingoid horses (hyperadrenocorticism) or horses on steroid treatment will also have delayed healing.
Age of the wound
Not all wounds are identified immediately. Maggots and granulation tissue do not happen in the first 24 hours. Older wounds may also have been treated with various topical agents. Many agents damage epithelial cells and increase the likelihood of delayed healing.
Key Takeaways
Healing can take quite awhile in many situations. Owners need to be well informed to better make decisions and plan. The most common factors that slow healing are lack of skin covering leading to proud flesh, bone surface damage leading to sequestration, and extensor tendon damage leading to a few days of required splinting.
Resources
See the following sections for management.
Wound Management: Wounds with Special Challenges, VCNA Vol.34(3), pp.511-538, 2018
Emergency Conditions in Horses: Opinions and Decision Making of Livery Yard Owners, Vet Evidence 2019
Factors that Affect Equine Wound Repair, VCNA Vol.21(1), pp.33-44, 2005
pieces of dead bone that cause persistent draining tracts as the body tries to liquefy them
proud flesh; granulation tissue that doesn't stop when the wound is filled but continues to grow into a mound
sutured edges come apart; lack of healing of incision
the inability of the animal to retract the penis back into the sheath
