Female urogenital surgery
How to – Urethral extension
Indications
Urethral extension is indicated for urine pooling that does not respond to Caslicks and/or perineal body transection. There are multiple techniques.
Relevant anatomy
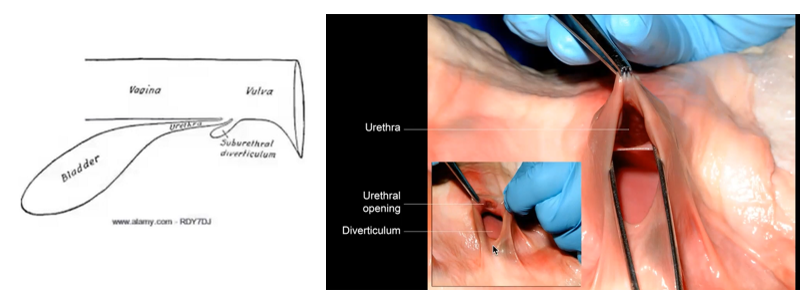
The urethra opens on the floor of the vaginal, approximately 6″ from the vulvar lips. The floor of the vagina is used to create a new tunnel.
Preoperative management
Food restrictions:NA
NSAIDs/analgesics:NSAIDs are recommended preoperatively.
Antibiotics: Antibiotics are generally considered optional. If used, trimethoprim sulfa is fine in horses. Ceftiofur or penicillin could be used in cattle.
Tetanus prophylaxis is recommended in horses
Local blocks: Epidural +/- splash block
Position/preparation:
The patient is restrained in a standing position and sedated as needed. The surgeon wears sterile gloves and uses sterile gel lubrication to ease manipulation within the vagina.
The tail is tied to the side, the rectum is emptied and the perineal area cleaned.
Pass a urinary catheter or foley into the urethra. The bovine urethral opening is tightly closed unless the cow has just urinated. The opening is approximately wrist deep, just past the blind urethral diverticulum. The tissue just beyond the diverticulum is actually two layers and is the opening of the urethra. Sometimes a urethra papilla can be palpated on the floor. Push forward and down over the papilla.
One suggestion – pass your finger and the catheter into the fold. Lift up and keep pushing the catheter forward. Can also try flipping so the catheter is on top. Alternate- pass your finger into the diverticulum to block it.

Surgery Supplies:
- Urinary catheter
- Scalpel and scalpel handle
- 0 suture, taper needle
- 2-0 suture, taper needle
- Needle holders
- Metzenbaum scissors
- Suture scissors
- Speculum or stay sutures
- Headlamp
- Allis tissue forceps – optional
- New methylene blue -optional
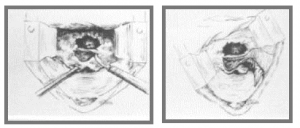
Surgical procedure – Shires & Kaneps
The vaginal vault is held open by stay sutures on the vulvar lips or use of a speculum. The floor of the vagina is loosely tacked up over the catheter using 2-3 horizontal mattress sutures of 0 suture material. The goal of this step is to hold the tissue in place; a water tight seal is not needed. Leave the suture ends long in case removal is needed.
The top edges of the tented tissue is transected using Metzenbaum scissors. This creates a fresh edge.
The fresh edges are apposed using a simple continuous pattern with 2-0 absorbable suture material.

The catheter is removed. If the tunnel is tight, the horizontal mattress sutures can be cut free.
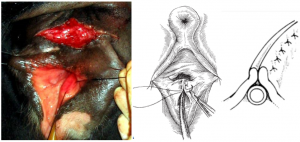
Surgical procedure – McKinnon & Vasey
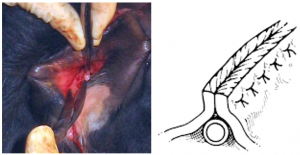
After gaining exposure of the vaginal vault, the transverse fold is grasped with Allis tissue forceps, retracted caudally and split into dorsal and ventral shelves using scalpel dissection horizontally across the fold. The dissection is continued on the vaginal walls, creating a flap of tissue on either side. Each flap should extend to the vulvar labia. The dissection is continued until both flaps can reach past the midline without tension. It can be challenging to determine where the dissection is complete due to the bleeding involved. Sterile new methylene blue dye can be used to aid in visualization of what is already dissected as the dye sticks only to the submucosal tissues.
The three flaps are opposed using a Connell pattern (full thickness Cushing).

Additional variations on this technique exist, including further dissection of the transverse fold so that the top layer can be pulled forward and cover the sutured Y part of the repair.
![]()
Postoperative care
- NSAIDs should be continued for 3 days
- The patient should be monitored to ensure she can urinate without difficulty
Complications
- Fistula formation is relatively common. Depending on the size of the fistula, repair may not be necessary
Videos
Resources
Shires and Kaneps, A practical and simple surgical technique for repair of urine pooling in the mare, AAEP circa 1989
Hooper and Taylor, Urinary Surgery. VCNA 1995, Vol.11(1), pp.95-121 – alternative technique pg 117-118; alternative link
