Swine, SRC, and poultry musculoskeletal disorders
How to – Hindlimb amputation
Indications
Limb amputation is recommended when the limb is painful and unlikely to improve, vascular supply is damaged, deep structures are infected, or when orthopedic stabilization is not possible (comminuted fractures, etc). In most cases, prostheses are not used. This description is for management of the animal when a prosthetic limb is not planned.
Relevant anatomy
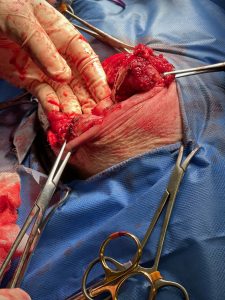
The hindlimb is amputated by removal mid-femur with this description. The limb may also be removed by disarticulating the coxofemoral joint.
.
Preoperative management
Food restrictions:
The procedure is performed under general anesthesia. Food should be withheld for 48 hours whenever possible.
NSAIDs/analgesics: Preoperative and postoperative analgesics are recommended.
Antibiotics: Not usually required.
Local blocks: Consider an epidural for pain management
Position/preparation:
The animal is positioned in lateral recumbency with the affected limb uppermost. The entire limb should be draped.
Surgery Supplies:
- Standard surgery pack
- 2-0 absorbable suture, taper needle
- 2-0 nonabsorbable suture, cutting needle
Surgical procedure
- Using the scalpel blade, create a slightly curvilinear incision extending from the fold of the flank, across the junction between the proximal 2/3 and distal 1/3 of the femur and up towards the ischial tuberosity.

- Create the medial incision 2 cm distal to the inguinal crease.
 Major veins and major arteries are double ligated with 2-0 absorbable suture. These vessels should be ligated separated to avoid the formation of an arteriovenous fistula.
Major veins and major arteries are double ligated with 2-0 absorbable suture. These vessels should be ligated separated to avoid the formation of an arteriovenous fistula.- When possible, transect through a tendon of insertion to minimize hemorrhage. As muscles are cut, hemostasis should be managed with electrocautery or ligation.

-
- Nerves are pulled gently distally and then severed. The nerve ends are allowed to retract naturally. Extension traction or crushing should be avoided.
- Elevate the limb. From the medial aspect, use transfixation sutures to doubly ligate the femoral artery. Transect proximal to the proximal caudal femoral artery. Ligate and transect the femoral vein.
- Transect the medial muscles at the level of the distal femur.
- Reflect the biceps femoris muscle and quadriceps muscle bellies to expose and transect the sciatic nerve.
- Transect the semimembranosus and semitendinosus muscles at the midfemur level. Repeat for the medial muscles.

- Sever the adductor at the midfemur level and elevate subperiosteally from the femur.
- Transect the femur using gigli wire at the junction between the proximal 1/3 and distal 2/3 of the bone.
- incise the periosteum circumferentially
- cut the bone transversely (oscillating saw or bone cutters may be used instead of gigli wire)
- smooth the end of the bone with a file
- lavage to remove fragments and bone dust

- Suture the cranial muscles (cranial sartorius, quadriceps, and biceps femoris) to the caudal muscles (semitendinosus, semimembranosus, gracilis and caudal sartorius muscles)
- Drains may be placed in dead space
- Trim excessive skin if needed. Avoid both excessive tension and excessive skin.
- Suture the skin using 2-0 nonabsorbable suture, avoiding having the incision run directly over pressure points such as the ischium. Start by apposing the skin flaps with interrupted sutures. The remaining closure can be performed using any appositional skin suturing pattern.
- Apply an elastic compression bandage to minimize edema and eliminate dead space.
Postoperative care
- The bandage is typically changed daily for 3-5 days.
- Assist the patient with standing and walking until they are able to do so without placing pressure on the amputation site
Complications
- hemorrhage
- minor hemorrhage can be controlled by a pressure bandage; more substantial hemorrhage will require repeat anesthesia/surgery and ligation of the bleeding vessel
- infections
- treat with hot packs and drainage
- skin ulceration
- treat with hot packs, excision of ulcerated tissue, and wound closure without tension
Videos
Video link – dog with osteosarcoma
Video link – feline amputation
Resources
Canine pelvic limb amputation, Clinician’s brief, 2021 Howard et al
