Equine and Camelid Castration
How to – Equine Castration, Recumbent
Indications
Equine castration is performed to remove the aggression and attention deficits associated with stallions.
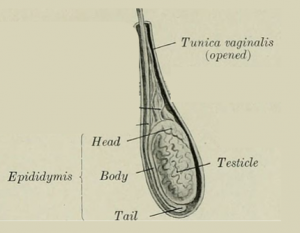
Relevant anatomy
Preoperative management
Food restrictions:
Ideally, food should be withheld for 6 hours. This is rarely performed but a heavy meal should be avoided.
NSAIDs/analgesics:
Preoperative NSAID administration is indicated to minimize pain and inflammation. Postoperative NSAID administration is strongly recommended for 3 days, longer if complications. Common choices are flunixin meglumine or phenylbutazone.
Antibiotics:
Preoperative antibiotics decrease complication rates. Procaine penicillin G or Excede are commonly used and are similarly effective.
Tetanus prophylaxis is required.
Local blocks:
Cord blocks are more challenging but more effective; lidocaine can also be injected directly into the testicle. Intra-testicular mepivacaine is likely to be more effective at relaxing the cremaster muscle.
Position/preparation:
Lateral or dorsal recumbency under general anesthesia (xylazine/ketamine/midazolam/GG or similar combination). Lateral recumbency is better for lung ventilation and can be done with fewer people. The upper hindlimb should be pulled forward to expose the testicles. 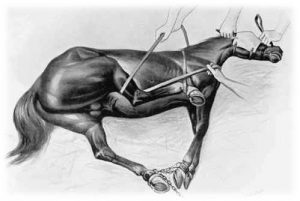
Dorsal can make it easier to identify and remove small testicles. Assistance is required for dorsal recumbency.
The scrotum is scrubbed and rinsed with alcohol before and after the local block is performed.
The surgeon cleans hands, applies an alcohol based sanitizer and gloves.
Surgery Supplies:
- Emasculator
- Scalpel blade
- Suture (0 absorbable, avoid chromic gut)
- Sterile gauze
- Scissors
- Forceps – carmalts and kellys
Surgical procedure –
narrated version (9:45 min) – video on youtube
Surgical procedure- written version
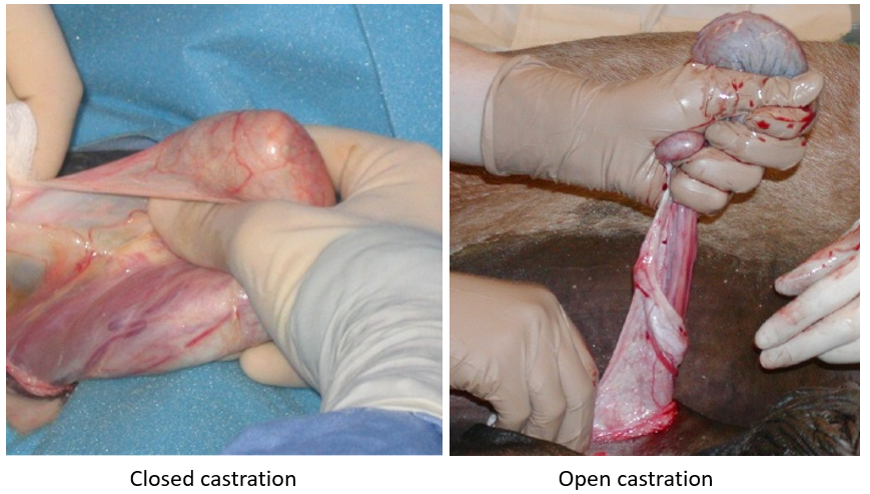
After both testicles are identified, the smaller or ventral testicle is removed first to ensure it is a testicle and to make it easier to remove to the second testicle. The testicle is stabilized and an incision made the full length of the testicle along its vertical axis down to the testicle. For an open castration, the tunic is opened and the testicle should pop out. For a closed castration, the tunic is not opened.
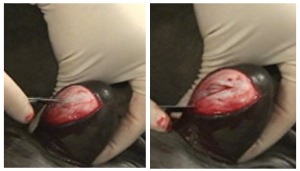
Dry gauze is used to strip the fascia from the testicle.

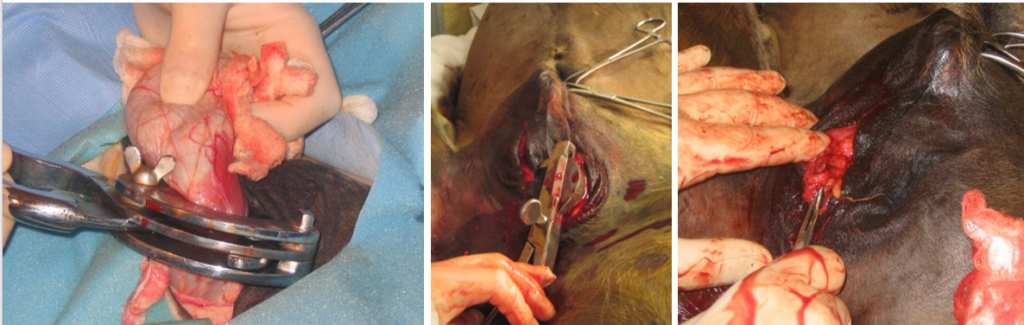
With open castrations, the cremaster muscle can be cut or emasculated (emasculation is quick, easy and minimizes bleeding). Additionally, the ligament to the tail of the epididymis is torn or cut with scissors. The cord is tagged (grasped at the edge) with a hemostat to enable it to be recovered if bleeding is noticed. Avoid crushing vessels with the hemostat; that confuses the issue later when you want to make sure you have a good crush or ligature.
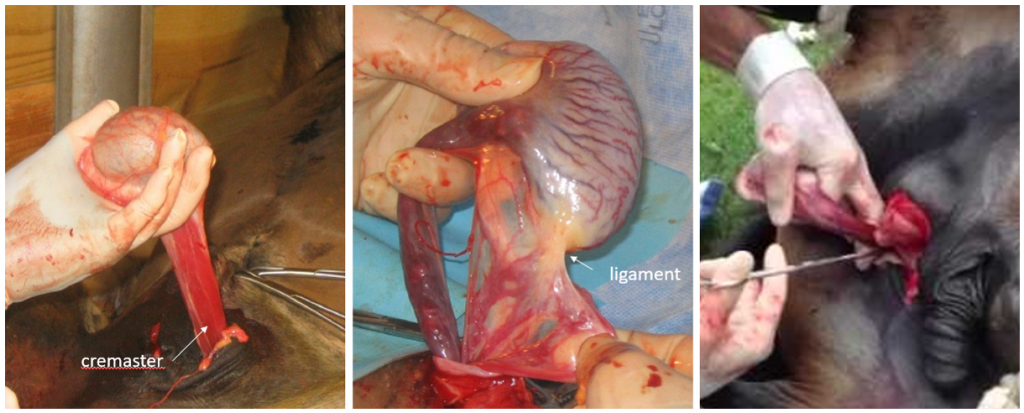
Optional : place a ligature (strangle knot, Millers, transfixation ligature) as far proximally as possible on the cord. This is much more difficult with closed castrations – note below how far the testicle can be exteriorized from the body in an open versus closed castration.
Place the emasculators on the cord, making sure to be at least a few centimeters distal to ligature. The emasculators are placed “nut to nut”, meaning the wingnut on the emasculator is adjacent to the testicle. This placement should ensure we have a crush proximal (on the body side) to the cut. Verify no skin is caught in the emasculators. Relax the testicle so there is no stretch on the vessels that would impair hemostasis. Crush firmly and completely. Leave the emasculators in place while you remove the second testicle or for at least 1 minute for yearlings, 2 minutes for older horses. The testicle can be transected distal to the emasculators if it is still connected.
Repeat for the second testicle.
As the emasculators are removed, check for bleeding. Ligate or recrush if needed. Remove the hemostats and check again for bleeding.
Stretch the incisions to ensure good drainage. Optional : cut the median raphe so that if one incision closes, drainage is still possible. Note: this usually wakes the horse up.
Clean up the patient, replace the halter and recover.
Postoperative care
- No food until awake, then feed a normal ration
- Stall rest until the following day. Then pasture turnout with forced exercise for 20 minutes per day or more.
- Continue NSAIDs for 3 days.
- Monitor for swelling, arterial bleeding, eventration or off feed (fever). The wound should drip constantly for at least several days.
Complications
- swelling
- facial or radial nerve paralysis
- infection
- eventration/evisceration
- hemorrhage
- hematoma if scrotum closed
- penile trauma if mistaken for a testicle
Videos
Video on youtube. Note his “modified closed” technique is really an open castration and a better option vs modified closed (7:50 min)
Video on youtube. Student castration lab (1:47 min)
Resources
You will find many contradictions and old wives tales in the literature, in practice and in the videos. These two articles “win” as far as being the most sound and evidence based. Start here for most efficient use of your time:
- New: Castration complications: A review of castration techniques and how to manage complications. VCNA (2021): 37:259-273
- Note- Please continue NSAIDs for 3 days postoperatively and most horses that develop infections due to premature scrotal closure do not need antibiotics, just drainage.
- Option: Equine castration : A review of techniques, complications and their management. Equine Vet Educ (2013): 25(9): 476-482
Intratesticular mepivacaine versus lidocaine in anaesthetised horses undergoing Henderson castration, Equine Vet J 2020;52:805–810
Equitwister, 2015 AAEP
Equitwister use :https://youtu.be/Z5nHQZjzzSY
Video compilation : good, bad and ugly
put out into a fenced yard; the opposite of being kept in a stall
