Equine Lameness
How to – Nerve and joint blocks
Local anesthesia is used to numb a region to determine if it is a source of pain. Blocks can be performed perineurally (around the nerve) or into synovial structures (joints, bursae and tendon sheaths). Typically we start low on the limb and work upwards. We try to keep moving up the limb before the prior blocks have worn off. Perineural blocks are usually less risky than intra-articular blocks. Intra-articular blocks carry the risk of synovial infections and needle breakage but the risk of infection is the same in the field as compared to in the hospital as long as proper cleaning and technique is used. Intra-articular therapy with steroids or other other agents may also be affected (increased risk of infection, decreased duration of action) by recent local anesthesia.
Perineural blocks are typically performed on both medial and lateral branches in the lower limb. Higher on the limb, the nerve may be blocked before it branches. The most common blocks are the palmar digital nerve block and the abaxial sesamoid nerve block. For perineural blocks, the skin is cleaned and smaller (22g, 25ga) needles used to place local anesthetic near the nerve. For intra-synovial blocks, the skin is prepped as for surgery and larger (18ga) needles are used to inject local anesthetic into the synovial cavity.
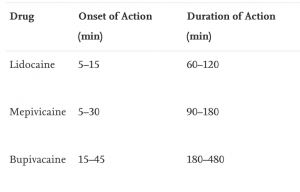
Mepivicaine is typically used for local blocks. It acts quickly (within about 10 minutes) and lasts ~2 hours. Lidocaine starts to act quickly (in about 2 minutes) but also wears off quickly (sometimes within the hour). If the local anesthesia wears off before the lameness is fully localized, things get very confusing. For example, if the horse improved 50% with a palmar digital block but you are still trying to get to 100%, you need that block to stay working. Bupivicaine is very long lasting (3-6 hours) and more tissue toxic. It is usually reserved for pain relief with laminitis or fractures, rather than for lameness evaluation.
Perineural blocks are assessed by checking the related skin sensation with a pen or pen cap. Eg a palmar digital nerve block should numb the skin of the heel bulbs but not the skin of the dorsal coronary band. The pen cap is used to see if the horse has lost sensation over the heel bulbs but still responds to pressure on the dorsal coronary band (the expected response). Joint blocks don’t have related skin sensation but joint fluid may be seen in the needle hub and the injection should flow smoothly with minimal pressure. Both types of blocks are checked at 10 minutes. Perineural blocks can be checked at 5 minutes; joint blocks may be reassessed up to 30 minutes or longer as the local anesthetic diffuses through and out of the joint.
Horses are typically blocked without sedation as most drugs alter the gait and alter the lameness exam. Twitches and good restraint are used along with careful positioning and attention to horse limbs to avoid trauma to the veterinarian.
Palmar digital nerves
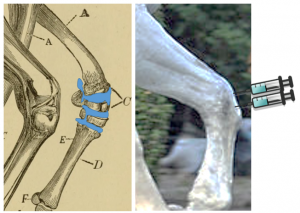
The neurovascular bundle is a group of structures that you can “strum” in the midpastern region on the palmar aspect. We usually try to block this bundle as low in the region as possible. A 25ga needle is used to inject local anesthetic subcutaneously around the nerve. When palpating the bundle, remember the nerve is closest to midline (axial). See yellow structure below.
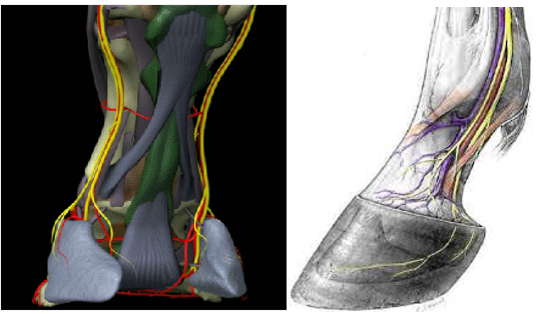
To desensitize heel region and sole, block both medial and lateral branches of the palmar digital nerve.

This block numbs the foot except for the dorsal laminae and dorsal coronary band. The area numbed includes the navicular bone, coffin joint, bursa, caudal heel region and sole. The numbed caudal heel includes the impar ligament, navicular suspensory ligament, collateral cartilages, frog, digital cushion and part of the deep digital flexor tendon. The PDN block does not always fully block the collateral ligaments of the coffin joint. It is important to know what is blocked and what isn’t blocked.
Coffin (DIP) joint
The coffin joint can be injected in a variety of sites:
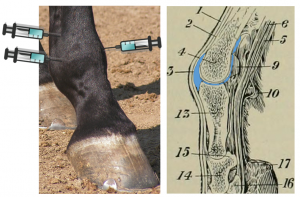
- Thumbs’ width above the coronary band and thumbs’ width off dorsal midline to either side: find a depression adjacent to the extensor tendon. Insert 20 ga needle either medial or laterally, angling to opposite corner of foot (eg if lateral stick, aim toward the medial heel). The needle should sink into a “hole” and it should be easy to inject fluid.
- On the lateral or medial aspect of the foot, one thumbs’ width above the coronary band (dorsal to the collateral cartilages), aim toward the center of the foot. Again, the needle should sink into a hole and it should be easy to inject the drug.

This block numbs the coffin joint, parts of the coffin bone, the coffin joint collateral ligaments, the impar ligament and the navicular bone. Over time, the local anesthetic diffuses out to block the navicular bursa and the caudal portion of the foot (coffin bone, soft tissue structures in the heel).
Equine coffin joint injection (Kaltura version w/ captions)
Navicular bursa block
To block the bursa, a spinal needle is inserted between the heel bulbs, parallel to the sole of the foot. Using contrast dye added to the local anesthetic, the needle location is checked radiographically before and after injection. The dye lets us verify what was blocked and also helps identify adhesions and loss of cartilage on the navicular bone.
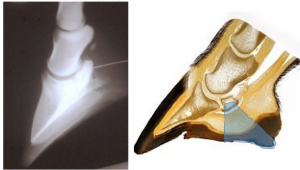
This block numbs the navicular bursa, the navicular bone and the caudal portions of the heel.
Pastern (PIP) joint
This joint is accessed very similarly to the dorsal coffin joint approach but just a little higher on the limb. Find the widest part of the long pastern bone (P1) and go just below this area. Insert a 20 ga needle just under extensor tendon, superficially into joint pouch ( you don’t need to get between bones). The joint can also be injected with the limb flexed : find “V” shaped notch at palmar distolateral aspect of the limb and aim the needle slightly distally and dorsally through this V. .

This block numbs the pastern joint. With time it can diffuse out and also act as a PDN block.
Basisesamoid nerves (abaxial nerve block)
The same neurovascular bundle as was used for the PDN block is readily palpable as it courses over the sesamoid bones. The nerve remains most axial. A 25ga needle is used for subcutaneous injection in area of nerve. Both medial and lateral branches are blocked to desensitize foot and pastern.

This block numbs the foot and the palmar/plantar aspects of the pastern.
Fetlock joint
The fetlock joint can be blocked using a variety of approaches:
- Insert 20ga needle in lowest area of the rectangle formed by splint bone proximally, cannon bone dorsally, suspensory ligament palmarly (plantarly) and sesamoid bones distally. The needle should be parallel to ground if the horse is weight-bearing. Injects easily.
- Insert 20 ga needle under extensor tendon dorsally (shallow injection into joint pouch).
- Insert 20 ga needle between cannon bone and sesamoid bones when joint flexed
This block numbs the fetlock. Over time it can also act like an abaxial sesamoid block.
Fetlock joint injection – video
Low 4 point/ low volar nerve block
For this block there are four nerves to block: deep and superficial branches on both the medial and lateral aspects of the limb. The deep nerves course between the splint bones and the cannon bone on the axial surface of the splint bones. These are blocked just distal to the end of the splint bone using 25ga needle. The superficial nerves course between the suspensory ligament and the deep flexor tendon but can be on either side of a fascial reflection: to block these, you need to fan the needle (move it around) with sufficient local anesthetic to cover a moderate sized area.

This block numbs the fetlock and distal cannon bone (palmar or plantar aspect).
High 4 point/ high volar nerve block
This block is very similar to the low volar block but performed above communicating branch. You can also inject all but the deep medial branch by injection between distal aspect of accessory carpal bone and cannon bone.

This block numbs the fetlock and more of the cannon bone and below. It can also numb the suspensory area and distal carpus or hock joints.
Carpal joints
To inject this joint, start by flexing the carpus. Note the 4 indentations. The indentations lie on either side of the wide tendon of the extensor carpi radialis m. that runs vertically over the dorsal aspect of the carpal joint. Inject above the proximal row of carpal bones to block the radiocarpal joint; inject above the distal row to block the intercarpal (midcarpal) joint . The intercarpal joint communicates with the more distal carpometacarpal joint so you do not need to block the carpometacarpal joint directly.
Video -carpal joint injections
Tarsometatarsal joint
On the lateral aspect of leg, follow the splint bone up until you reach a flat, thumb sized area (slight depression). This flat area is above the tarsometatarsal joint (it helps if you can find a skeleton). Insert a 1″ 22ga needle slightly distally and slightly dorsally until it sinks its full length into a hole.
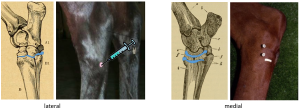
This joint can also be injected medially in a very small depression on the distal aspect of the cunean tendon.
Distal intertarsal joint block
On the medial aspect of hock, find small depression on proximal aspect of the cunean tendon; insert 22ga 1″needle into the space, parallel to the ground (see upper needle on image above).
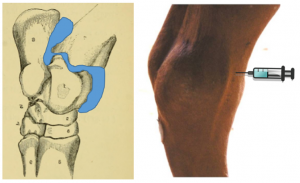
Tibiotarsal joint
To inject the tibiotarsal joint, inject on either side of saphenous vein on dorsal aspect of leg using 20 ga needle parallel to ground
Videos of hock joint injections
Tibial/peroneal nerve block
Tibial nerve: Palpate the calcanean tendon about 4″ above point of hock, insert 22ga needle under the tendon from the lateral side. Push the needle until its point can be felt just under skin medially. Inject.
Peroneal (fibular) nerve: at same level as the tibial nerve block, inject on lateral aspect of leg between the muscle bellies; fan local anesthetic.
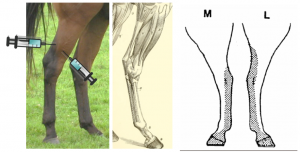
This block can numb the hock and the plantar surface of the distal limb. These blocks can also be performed using ultrasound guidance.
Resources
Diagnostic analgesia of the equine distal limb, UGA free ibooks
General info about joint injections – video
Local anaesthetics for regional and intra-articular analgesia in the horse, Equine vet. Educ. (2021) 33 (3) 159-168. Review article
Manual of Clinical Procedures in the Horse Ch 28
Where does it hurt? Problems with interpretation of regional and intra-synovial diagnostic analgesia, 2015 EVE
Injecting the stifle video
Equine Joint Injection and Regional Anesthesia Spiral-bound – Useful resource for practice
