Eye surgery
How to – Eyelid laceration repair
Indications
Eyelid lacerations require primary closure or exposure keratitis is likely.
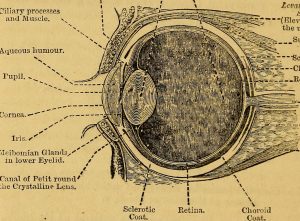
Relevant anatomy
The eyelid margin includes meibomian glands and eyelid musculature.
Preoperative management
Food restrictions: NA. These are treated as an emergency
NSAIDs/analgesics: Preoperative NSAIDs are necessary for swelling management.
Antibiotics: Preoperative antibiotics are recommended.
Tetanus prophylaxis is recommended for horses.
Local blocks: The palpebral nerve is blocked to allow eyelid manipulation but does not provide analgesia. The supraorbital nerve is blocked to provide analgesia to the upper lid. Lower lid lacerations are usually blocked with regional anesthesia.
Position/preparation: Patients may be standing or under general anesthesia. Stacked haybales (covered with a blanket) or a dental stand can be useful to hold the head steady at an appropriate level. Eye lube is used to protect the cornea. The area is prepped using betadine solution rather than scrub. Avoid chlorhexidine (toxic to the cornea) and alcohol. Use saline to remove the betadine. The eyelashes may be trimmed if needed but rarely is further clipping required. Surgeons glove.
Surgery Supplies:
- Standard surgery pack
- 3-0 or 4-0 soft suture material, cutting and taper needles
- headlamp or surgery lighting
Surgical procedure
- Minimal to no debridement. Skin loss prevents eyelid reconstruction
- The subconjunctiva can be closed if accessible. Simple continuous pattern of 4-0 suture with knots placed superficially (away from the cornea).
- The eyelid margin is carefully reconstructed. The figure 8 pattern avoids suture knots on the cornea.
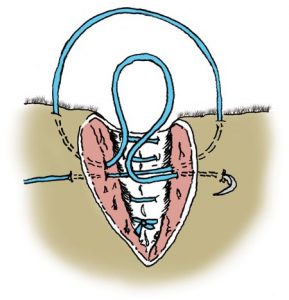
To do this pattern well, it is important to keep all bites very symmetrical. The bites crossing the top of the laceration exit/enter the area of the meibomian glands. The suture ends can be left a little long and then folded under adjacent suture to keep the ends away from the cornea.
The lid margin of the llama below was too uneven; this will cause corneal issues. The suture was removed and redone to better appose the laceration edges.

Once the eyelids are apposed, the remainder of the laceration can be closed routinely.
Postoperative care
- NSAIDs are continued for 3-5 days
- Patients should not be allowed to rub the eyes
- Suture removal in 10-14 days
Complications
- Corneal injury can occur related to the original injury, related to the surgery and/or to suture or tissue rubbing on the cornea
- Dehiscence
Videos
Figure 8 pattern using a lip as a bigger model
Resources
J Gionfriddo. Skills Laboratory: Eyelid laceration repair: A step-by-step guide. DVM 360
A Dwyer. Ophthalmic emergencies in the field, 2021 VCNA Vol 37; pp 441-460
sutured edges come apart; lack of healing of incision
