Food Animal Male Urogenital Surgery
How to – Unilateral castration
Indications
Unilateral castration is most commonly performed to maintain fertility in a male animal despite trauma, tumors or temperature changes in the single testicle. Inguinal hernias are treated most effectively by unilateral (if not bilateral) castration. Removing the testicle means being able to fully close the inguinal ring. Leaving space for the testicular artery means leaving space for the guts to come through, as well.
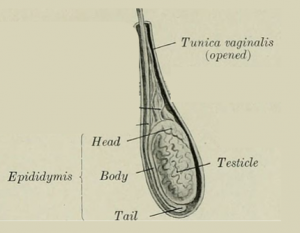
Relevant anatomy
Preoperative management
Food restrictions: In bulls, the procedure can be done standing in a chute with no sedation. In most other cases, the animal is only lightly sedated for the procedure and no food withholding is required. If needed for exotic ruminants or other cases, food should be withheld for 48 hours to minimize bloat.
NSAIDs/analgesics: Preoperative NSAID administration is recommended to minimize pain and inflammation. Postoperative NSAID administration is indicated. Excessive inflammation can lead to fibrous tissue formation and inability to thermoregulate.
Antibiotics: Antibiotics are not usually indicated unless the reason for castration involves infection. Results of culture and sensitivity can guide antibiotic selection if available. If not, the most common organism in cattle will be Trueperella pyogenes. Antibiotics tend not to work well in pus despite sensitivity in vitro. Drainage is important.
Tetanus prophylaxis is recommended.
Local blocks: Lidocaine is used to block the cord and/or the surgical site. A cord block avoids distortion of the surgical site. A ring block around the cord can help with analgesia.Injection along the proposed incision line and into the testicle is quick and effective but does alter the anatomy.
Position/preparation: Bulls can be restrained a chute with a butt bar in place. Sheep are held in a sitting position. Other animals are cast or sedated until in lateral recumbency. The upper leg should be pulled forward to expose the scrotum. The scrotum is clipped (if needed) and scrubbed prior to and after the local block. Surgeons should glove.
Surgery Supplies:
- Scalpel blade + handle
- Needle holders
- Suture scissors
- 0-1 absorbable suture depending upon patient size
- Emasculators
Surgical procedure
An incision is made vertically in the scrotum, following the length of the affected testicle along its abaxial border (minimizing trauma to the unaffected testicle). The testicle is exteriorized. The cord is ligated with 0 absorbable suture (avoid chromic gut). The testicle is emasculated distal to the ligature or another ligature placed.
The scrotum can be left open for second intention healing if infection is a concern. Betadine soaked gauze can be inserted into the space to keep the wound open until the space is closed by granulation tissue. Animal comfort is increased if the scrotum can be closed. Extra skin can be removed to minimize deadspace but will cause bleeding. The scrotal skin is closed with simple continuous, cruciates or a Ford-Interlocking pattern. Two -three interrupteds placed ventrally will make drainage easier if infection develops. Absorbable suture may be used if removal will be difficult.
Postoperative care
- Continue NSAID therapy for 3 -5 days
- Cold hydrotherapy can be used if the skin was closed and if swelling is present.
- If packing was used, pull out and trim off a small amount each day until fully removed.
- Keep the area clean and dry for 10 days postoperatively
- Minimize exercise for the first day to minimize the risk of bleeding
- Monitor for signs of infection, herniation or dehiscence.
- Evaluate semen quality in 60 days (allow recovery).
- Communicate meat withholding restrictions
Complications
Inflammation can cause scarring. Scarring can lead to inability to thermoregulate and subsequent infertility.
Videos
Video link– hemicastration
Resources
Abnormalities of the scrotum and testes, 2024 VCNA
