FA GI Topics
How to – Right flank omentopexy/antropexy
Indications
Stabilization of the abomasum is indicated with any DA surgery and is generally performed any time a right flank exploratory is performed (prophylactic tack). Right flank omentopexy is one option. Omentopexy combined with a tack of the antrum (often called pyloropexy) is a modification that may be stronger.
Relevant anatomy
The abomasum is normally located on the ventral abdomen, typically just to the right of midline. It often shifts horizontally across the midline during late gestation. When gas filled, the abomasum can displace to either the left or the right sides of the abdomen and float up. The pylorus will stay more ventral while the body of the abomasum floats more freely upward.
The greater curvature of the abomasum is encased within the omental bursa – a potential space formed by the greater and lesser omentum (omental leaves). The greater omentum has two layers. The superficial layer connects the descending duodenum, abomasum and the left longitudinal groove of the rumen. The deep layer connects the duodenum, abomasum and the right longitudinal groove of the rumen. This creates the “sling” and the omental bursa between the layers. The lesser omentum connects the abomasum, liver and ascending duodenum.
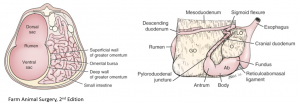
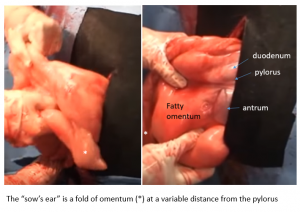
The abomasal antrum is visible while the pylorus and proximal duodenum are encased in omentum. The “sows ear” is not necessarily close to the antrum.
The flank musculature is comprised of the external abdominal oblique, internal abdominal oblique and transversus abdominus muscle.

Preoperative management
Food restrictions: NA
NSAIDs/analgesics: Recommended preoperatively. Flunixin meglumine 1.1-2.2 mg/kg iv is standard.
Antibiotics: Recommended. As cows can wall off infection, there can be surprises inside. If the cow is milking, ceftiofur 2.2 mg/kg im is standard. In beef or non-lactating cattle, other options do exist. Remember: the label dose of procaine penicillin is ineffective!
Local blocks: A line block, inverted L or paravertebral are all reasonable options.
Position/preparation: See How to- Standing GI Surgery
Surgery Supplies – Additional
- 2 chromic gut, 2 vicryl, 2 nylon or similar for the pexy
- DA simplex – long flexible tubing attached to a 10ga needle for viscus decompression
- 0 vicryl or similar for the abomasotomy with abomasal volvulus
- Large bore stomach tube – only if abomasal volvulus
Surgery Supplies- Standard
- Standard surgery pack
- Sterile sleeves for internal palpation
- Scalpel blade and handle
- 2 or 3 absorbable suture material for muscle closure
- 3+ nonabsorbable suture material for skin closure
Surgical procedure
Follow the guidelines for Standing GI surgery. , How to – Abdominal Exploratory
To replace a left displaced abomasum
Identify the top part of the abomasum or as high as you can reach. Take the DA simplex (tubing with 10 ga needle attached) into the abdomen, protecting the needle by having it in your palm or folded backwards. When you reach the abomasum, tunnel the needle through the wall of the DA for a few millimeters and then direct it perpendicularly into the lumen. Push down on the abomasum to encourage as much gas as possible to escape. Kink the tubing and remove the simplex and drop it on the floor or hand to a nonsterile assistant (it is contaminated).
Reach under the omental sling and grab the pylorus OR grab the omentum that is in the cranioventral aspect of the abdomen and gradually pull toward you and then caudodorsally (see Fig 3) to pull the abomasum over to the left side. This may take some wiggling or manipulation inside the cow. If the omentum starts to tear (much more likely in very fat cows), stop and try to find the pylorus to pull the abomasum over directly. NOTE: Pulling vertically pulls on the rumen and pulling horizontally pulls on the duodenum and liver. Neither will help reposition the abomasum. Pull at an angle.
If the abomasum is not moving, check for
- excessive gas – re-palpate craniodorsally and repeat the gas removal if necessary
- adhesions – previous pexy or ulcer – palpate along the ventral body wall. If present, close the incision and move to plan B
- torn omentum – attempt to grab the pylorus itself
To replace a right displaced abomasum
Identify the gas distended viscus and verify displaced vs twisted. Run your hand down the medial aspect. If you hand can follow the medial aspect down to the ventral abdomen, it is just displaced. A twist will stop your hand midway down. A twist is also usually accompanied by displacement of the omental sling. If you have a twist, see below.
Decompress the abomasum using the tunneling technique + direct stab. Once the gas is relieved, dispose of the simplex and grab the pylorus. The abomasum has flipped up in a counterclockwise manner as viewed from the rear. Push down the body of the abomasum while pulling up on the pylorus. If you move too slowly, the gas will redevelop and you will need to repeat the decompression.
To correct an abomasal volvulus
With a volvulus, the abomasum has moved into the RDA position (flipped up) and then twisted counterclockwise as viewed from the right side of the cow. You need to twist it clockwise into RDA position and then flip it down. However, it is usually full of fluid. Untwisting can be challenging until you remove the fluid.
Cover both arms with sterile sleeves and add overgloves, set up abomasotomy instruments (needle holders, suture scissors, suture, blade) and move the clean instruments aside. Preplace two purse string sutures of 0 vicryl in the exposed abomasal body – one with a center diameter of 4 cm and one encircling that with a slightly larger central diameter. Leave the ends of each purse string long. Create a stab incision in the center, big enough for your large bore stomach tube. Quickly insert the stomach tube, passing it into the ventral aspect of the abomasum. Abomasal fluid will start to siphon off. Adjust the tube as needed to remove as much fluid as possible. Remember, as you pull the tube out, the tube is contaminated. Remove the tube fully and tighten the purse string sutures. Clean the surface and remove the overgloves and sleeves. Use the suture in the last purse string or an additional strand to cover the knots with an inverting pattern.
Reposition the abomasum by pushing it forward and then down (or pull on the pylorus clockwise and then correct the RDA).
Omentopexy
Prior to closure, palpate the abomasal wall for ulcers and perform the omentopexy. There are several viable methods. This is one of them:
Pull the abomasum up (or extend the incision down) so that the abomasal antrum is visible (Fig 1). Clamp the omentum dorsal to the antrum to the dorsal aspect of the incision to hold it in place. The pylorus should not be elevated more than necessary or it puts the cow at risk of duodenal torsion.
Place 2 horizontal mattress sutures across the cranial incisional musculature and the omentum + 1 horizontal mattress across the musculature and the antrum.
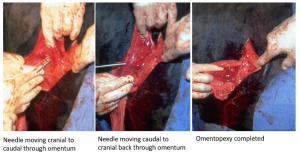
- Omentopexy bites: Starting on the external abdominal oblique using 2 suture material, insert the needle 1 cm caudal to the cut edge, through the internal abdominal oblique, through the transversus, through the omentum (the part that is just caudal to the pylorus or duodenum) from cranial to caudal, back through the omentum from caudal to cranial, back through the transversus, back through the internal abdominal oblique and back through the external abdominal oblique. Tighten up the suture so the omentum is tightly against the body wall. Tie. Repeat for 1-2 more sutures.
- Antropexy bite: Using the same process, insert the needle through the musculature, through the slipped wall (mucosa not included) of the abomasal antrum, back through the slipped wall of the abomasal antrum and back through the musculature. With an RDA, you may be able to get 2 horizontal mattress sutures in the antrum instead of just one.
Closure is as described in How to- Standing GI Surgery. If the internal abdominal oblique muscle slid away during the pexy, you cannot use it for closure. Attach the caudal aspect to whichever layer you prefer. One wound, one scar applies anyway. In 10 days, you can’t tell the difference.
Postoperative care
- Suture removal in 10-14 days.
- Monitor the cow for any signs of infection or peritonitis.
- Consider rumen transfaunation if available.
- If abomasotomy was performed to drain fluid, continue antibiotics for 5 days and NSAIDs for 3-5 days.
Complications
- Incisional dehiscence (rare)
- Incisional infection (common)
- Peritonitis
Abomasal volvulus
- Abomasal necrosis – if a portion of the abomasum is purple or if the purse string sutures pull out, the abomasum is devitalized. Quit.
- Abomasal atony – in some cases the abomasal wall is so stretched, it never works again. Cull.
- Unable to detorse – sometimes the omasum and/or reticulum are involved and detorsion is very challenging. Refer or quit.
Videos
Youtube videos (age restricted)
Resources
Farm Animal Surgery (Second Edition), 2017
Wittek T et al. Ultrasonographic assessment of change in abomasal position during the last three months of gestation and first three months of lactation in Holstein-Friesian cows. J Am Vet Med Assoc 2005; 227:1469-1475
tacking the omentum in place to prevent movement of the abomasum
suture pattern in which tissue edges are turned inward
