Bladder, Urethra and Ureters
How to – Tube cystotomy
Indications
Tube cystotomy is typically performed in small ruminants for treatment of obstructive urolithiasis. Tube cystotomy can be performed in other species. It is generally temporary but can be a permanent option if the obstruction does not resolve or is due to polyps or tumors.
Relevant anatomy
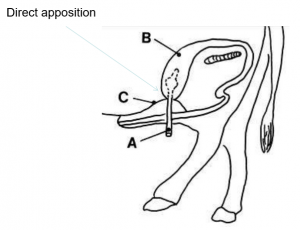
A tube is placed in the bladder and exited from the body wall in a location that allows the bladder to sit in a normal position and in direct apposition to the body wall.

Preoperative management
Fluid deficits and severe electrolyte abnormalities should be corrected preoperatively. Hyperkalemia is rare in goats and dehydration is not often severe so therapy does not often need to be completed prior to anesthesia.
Food restrictions: NA
NSAIDs/analgesics: Preoperative NSAIDs and analgesics are recommended as goats are very sensitive to pain. Flunixin meglumine is often combined with a narcotic.
Antibiotics: Preoperative antibiotics are indicated. Common choices are ceftiofur, amoxicillin or ampicillin.
Tetanus prophylaxis is recommended.
Local blocks: The skin incision can be blocked using a U shaped line block and a rectus sheath block can be performed.
Position/preparation: Dorsal recumbency
Anesthesia recommendations:
Induction with midazolam (muscle relaxation and sedation;.1-.2mg/kg), ketamine (5mg/kg IV), +/- opioid or additional ketamine
Consider inverted U block or TAP block
If in field, IM — less ketamine + local epidural, position goat to prevent aspiration of rumen fluid. Better to bring into the clinic
Watch metabolic derangements: hyperkalemia, watch for bradycardia
Surgery Supplies:
- Standard surgery pack
- 3-0 absorbable suture (bladder)
- 0-1 absorbable suture (PDS) or nonabsorbable suture (body wall)
- 2-0 absorbable suture (musculature, SQ tissue)
- 2-0 to 0 nonabsorbable suture (skin)
- 2-0 to 0 suture for fingertrap knot (braided works well to hold it but is often absorbable so can be a problem in long term cases)
- Pezzar (foley if pezzar is not available) sized to match the patient (no more than 1/8 size of bladder when not distended). Pezzars are preferred as the foley balloon can rupture. If used, the balloon should be distended with saline rather than air.

Surgical procedure
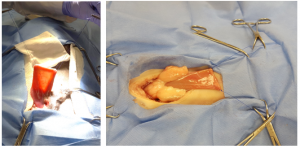
The patient is placed in dorsal recumbency under general anesthesia, prepped and draped.
A paramedian skin incision is made in the caudal abdomen, adjacent to the prepuce. The incision should extend ~10 cm and finish between the nipples. The skin and prepuce are shoved to the side and the abdomen opened through the linea alba.

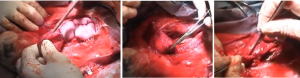
The bladder is identified. Two 3-0 stay sutures are placed in the bladder at the dorsal aspects on either side.
The bladder is incised close to the trigone and the bladder flushed to remove as many stones as possible. A red rubber catheter can placed into the urethra and the urethra flushed (low pressure only) to remove additional stones. Forceful flushing can easily rupture the urethra and should be avoided.
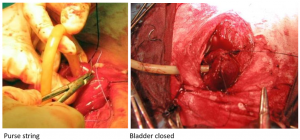
A second incision is made on the same side of the bladder as the tube will exit the body wall. A small nick is made and the tube passed through the nick. This can be done by pushing the pezzar end into the bladder or the tube end out of the bladder. A purse string suture is placed around the tube.
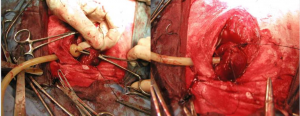

The bladder is closed in 2 layers using 3-0 absorbable suture in inverting patterns. The stay sutures can be tied in place in trimmed short to prevent leaks. The bladder should be checked for leaks by adding fluid through the pezzar.
The tube is exited through all layers of the body wall, generally at a slight angle so that there isn’t a direct path from body wall to outside but that each opening is a little off from the others. Be careful to make sure the tube goes through the wall, not through the incision (or you can’t close the incision). **The bladder needs to reach the body wall- the incision through the skin cannot be too far forward.**
The pezzar is pulled up so the bladder is snug against the body wall. The pezzar is secured in place using a fingertrap knot of 2-0 suture material. 
The body wall is closed routinely. The linea is closed using a simple continuous pattern with slowly absorbing 0 suture material. If the incision was off midline, the ventral sheath of the rectus abdominis is closed similarly. Subcutaneous tissues are closed in a simple continuous pattern using 2-0 absorbable suture. The skin is closed using nonabsorbable suture in a Ford interlocking or simple continuous pattern.
The pezzar is tacked to the body wall in 2-3 spots so that the opening of the pezzar is lined up with the preputial opening.

A tape butterfly suture can be useful to keep the tube from sliding

Have the tape extend to each side and tape back to itself so there are nonsticky tabs on either side. Pass suture through these to secure to skin of ventral abdomen.
Postoperative care
- A glove fingerip is placed over the end of the tube; a nick is made in the end of the glove finger to allow urine drainage. This is to minimize the risk of ascending infection.
- Postoperative analgesics are usually required in the first 24 hours. Buprenorphine is commonly used; morphine is also an option.
- The patient is left on antibiotics until after the tube is removed.
- NSAIDs are maintained for at least 3 days, typically until normal urine flow is resumed.
- The tube is checked frequently to ensure the tip is dripping. If dripping stops, the tube may be blocked by a stone or blood clot. The obstruction should be flushed free using sterile technique.
Most patients will start urinating out of the prepuce within a few days. Once the obstruction is relieved with the tube placement, the urethra relaxes and the stone(s) pass.
The tube should be left in place for at least 8 days. The goal of this time frame is to permit an adhesion to form between the bladder and the body wall so urine does not leak into the peritoneal cavity with tube removal.
Once the patient is urinating and it has been at least 8 days, the tube can be removed. The fingertrap knot is removed, the body wall is held in place with one hand while the tube is pulled forcefully with the other. The owner should monitor for uroabdomen (distension, off feed) but this is rare.
Complications
Lack of urination
Occasionally the stones do not pass. Lidocaine can be infused up the catheter using sterile technique. A lidocaine epidural may be administered. Muscle relaxants and alpha blockers (acepromazine, bethanechol, phenoxybenzamine) can be tried. The tube should be kept in place. Occasionally other therapy (laser lithotripsy etc) may be necessary.
Urethral rupture
If flushing is too vigorous, the urethra may rupture. The skin ventral to the area should be lanced and the tissues flushed. The tube will help with healing.
Infection
As with any surgery, incisional infections and peritonitis are a risk. Animals will be off feed, tender on palpation of the incision (incisonal infections), and may be febrile.
Videos
Goat cystotomy: Youtube video
pulling pezzar through body wall: youtube video
Resources
Urolithiasis in small ruminants, AASRP- more details than you ever wanted to know; good reference for future as he goes through more complex situations; please don’t do the hydropulsion though.
Surgery of obstructive urolithiasis in ruminants, VCNA 2008 -good overview with nice references; good for your files
Bladder stone removal (dog): youtube video
suture pattern in which tissue edges are turned inward
