FA GI Topics
How to – Typhlotomy
Indications
Typhlotomy is performed to quickly remove fermenting contents in cattle with enlarged ceca due to hypocalcemia and poor motility and with cecal displacements and torsions.
Relevant anatomy
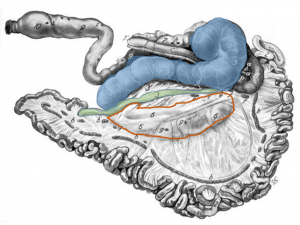
The cecum is a blind ended sac with the tip pointing caudally. It is connected to the spiral colon dorsally and to the ileum ventrally. It has no identifiable features on palpation in the abdomen but is usually found sitting on top of the viscera between the rumen and omental sling. When distended it is easier to find and will usually protrude out the incision. It can distend to up to 3 feet, creating a “ping” that runs the length of the abdomen below the transverse processes. It is not tacked to the body wall so can displace and can twist on its long axis.
Preoperative management
Food restrictions: NA
NSAIDs/analgesics: Recommended preoperatively. Flunixin meglumine 1.1-2.2 mg/kg iv is standard.
Antibiotics:Recommended. As cows can wall off infection, there can be surprises inside. If beef or non-lactating cattle, ceftiofur 2.2 mg/kg im is standard. In dairy cows, other options do exist. Remember: the label dose of procaine penicillin is ineffective!
Other: If the cow has signs of hypocalcemia (cold ear tips, slow PLR), calcium should be started.
Local blocks: A line block, inverted L or paravertebral are all reasonable options.
Position/preparation: See How to- Standing GI Surgery
Surgery Supplies- Additional
- Extra sleeves and gloves
- Additional laceration or surgery pack is ideal
- Sterile saline for lavage
- Sterile assistant
- Lap sponge forceps -optional
- 3-0 absorbable suture (taper needle) for typhlotomy
- DA simplex – long flexible tubing attached to a 10ga needle for viscus decompression -optional
- Biopsy instruments and formalin- optional
Surgery Supplies – Standard
- Standard surgery pack
- Sterile sleeves for internal palpation
- Scalpel blade and handle
- 2 or 3 absorbable suture material for muscle closure
- 3+ nonabsorbable suture material for skin closure
Surgical procedure
See How to- Standing GI Surgery and How to – Abdominal Exploratory
It may not be possible to complete the exploratory until after the typhlotomy but it should be attempted to minimize contamination risk.
Instruments should be separated into typhlotomy (will be dirty) and closure sets (should stay clean). The typhlotomy set should include a scalpel blade, sterile saline, gauzes, needle holders, suture, scissors and lap sponge forceps or large hemostats. The closure set (the rest of the instruments) should be covered to minimize the risk of contamination.

The surgeon and assistant surgeon should wear sterile sleeves and overgloves to ease clean up after the typhlotomy.
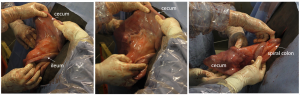
Exteriorize the cecum as much as possible.
The assistant is in charge of making sure the cecal contents and lavage fluid do not go into the abdomen. The assistant should hold the cecum near the tip but not at the tip. This will allow the assistant to direct the contents away from the abdomen and to keep the fluid flow downhill.
Create a 3-5 cm incision at the tip of the cecum. Use the sponge forceps or large clamp to pull out any obstructing chunks so the cecum empties as much as possible. Saline lavage can be provided by the sterile team or by an unsterile assistant.
Once the cecum is emptied, the assistant should elevate the tip of the cecum so that the incision is no longer ventral. This will minimize continued ingesta flow and keep the cecal incision clean for closure. The incision line is flushed gently (be careful of flush wanting to go back into the cow) and cleaned of any gross debris. The incision is closed with a double inverting pattern or a single continuous Lembert. It is important to ensure this line is tight. Midway through the pattern and at the end, hold the working end of the suture in your right hand and use the left to slide down the suture, pushing the sutured cecal tissue toward the suture knot. The cecum will gather slightly but leaks will be minimized. Once the closure is complete, the cecum is again cleaned and returned to the abdomen.
Occasionally the cecum will quickly refill. The incision can be opened and the process repeated.
The typhlotomy pack is covered or removed and the dirty sleeves and gloves removed. The remainder of the procedure can be completed as described in How to- Standing GI Surgery, making sure the cecum is in its normal position with the tip pointing caudally.
Postoperative care
- Antibiotics and NSAIDs should be continued for at least 3 days.
- Monitor calcium levels and for signs of peritonitis
Complications
- Peritonitis
- Incisional infection
- Continued motility disturbances
Videos
Resources
incision into the cecum
suture pattern in which tissue edges are turned inward
