LA Respiratory Issues
Guttural pouch disorders
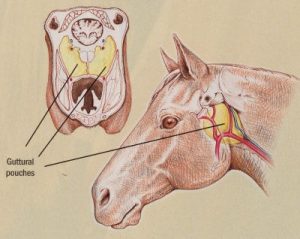
The guttural pouches are unique to a small number of species, including the horse. The guttural pouches are expansions of the Eustachian tube and are theorized to help with brain cooling. Diagnosis of guttural pouch disorders often includes endoscopy of one or both pouches.
Even though the openings are caudal to the nasal septum, discharge tends to remain unilateral unless severe or chronic. Why they don’t cause bilateral drainage isn’t entirely clear. Perhaps related to normal head position or the dorsal position of the openings?
Guttural pouch disorders can lead to hemorrhagic nasal discharge (mycoses, fractures) or purulent nasal discharge (empyema, chondroids). It is very useful to be able to create a differential list based on the type of discharge!
Guttural pouch disorders with surgical options
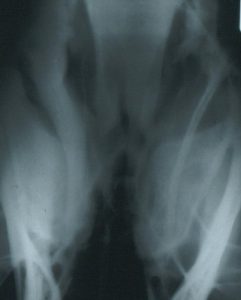
Guttural pouch empyema
 Guttural pouch empyema, or pus in the guttural pouch, is frequently related to strangles (Streptococcus equi infection). Affected horses are often infectious. Drainage from the guttural pouch openings may be seen on endoscopy. Treatment generally involves lavage of the guttural pouch combined with systemic and/or local antimicrobials. Antibiotics alone are not usually sufficient. Retropharyngeal lymph node swelling or full guttural pouches can compress the pharynx (“strangling” the horse). Tracheotomy may be needed.
Guttural pouch empyema, or pus in the guttural pouch, is frequently related to strangles (Streptococcus equi infection). Affected horses are often infectious. Drainage from the guttural pouch openings may be seen on endoscopy. Treatment generally involves lavage of the guttural pouch combined with systemic and/or local antimicrobials. Antibiotics alone are not usually sufficient. Retropharyngeal lymph node swelling or full guttural pouches can compress the pharynx (“strangling” the horse). Tracheotomy may be needed.
This radiograph shows a fluid line in the guttural pouch.
Clinical signs – bilateral purulent nasal discharge, fever, poor appetite, swollen lymph nodes
Guttural pouch chondroids
Chondroids develop when the purulent material from guttural pouch empyema desiccates. Inflammation of the guttural pouch causes disruption in mucociliary clearance and the horse is unable to clear the purulent material in the pouches. Overtime the pus become stone-like. These “stones” of pus may need surgery for removal. NO agents have been found to dissolve the stones and many compounds lead to severe trauma to the guttural pouch. Chondroids generally have to be flushed out or removed manually. This is not an easy process. Surgery may be necessary but has lots of risks due to the related inflammation that occurs near all sorts of named arteries and nerves. There is no easy ventral drainage of the guttural pouch. As most animals don’t have guttural pouches, this is a horse thing.
Clinical signs – unilateral or bilateral purulent nasal discharge, often without other signs
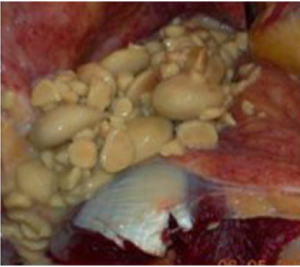
Chondroids in the guttural pouch of a horse. Source: Dixon et al. Equine guttural pouch empyema, why does it become chronic? Equine vet. Educ. (2018) 30 (2) 80-84
Guttural pouch mycosis
 Guttural pouch mycoses are fungal infections, generally involving Aspergillus fumigatus. This opportunistic fungus lives in the environment and attaches to an artery in the guttural pouch for nutrition. It can erode through the arterial wall, and involve different combinations of the internal carotid artery, external carotid artery and maxillary artery leading to bleeding (often severe, can be life threatening!). The horse usually presents with moderate to severe epistaxis bilaterally. If the fungus is on an artery, surgical occlusion of the artery is the preferred therapy. This requires both proximal and distal occlusion of the artery due to the Circle of Willis . The Circle of Willis is a circle of arteries around the brain. This loop leads to the potential for blood flow from both ends of the artery. Due to access issues, a balloon or coils are used to block off the far end of the artery while a ligature is used on the artery outside of the pouch. If the fungus is on a bone or non-arterial structure, it can be scraped off or treated with topical antifungals. Due to the risk of fatal hemorrhage, those options are not recommended for fungal infections involving an artery. Antifungal agents are not required if surgery is used, as the fungus cannot live without the arterial oxygen supply. Once the artery is occluded, the fungus dies off.
Guttural pouch mycoses are fungal infections, generally involving Aspergillus fumigatus. This opportunistic fungus lives in the environment and attaches to an artery in the guttural pouch for nutrition. It can erode through the arterial wall, and involve different combinations of the internal carotid artery, external carotid artery and maxillary artery leading to bleeding (often severe, can be life threatening!). The horse usually presents with moderate to severe epistaxis bilaterally. If the fungus is on an artery, surgical occlusion of the artery is the preferred therapy. This requires both proximal and distal occlusion of the artery due to the Circle of Willis . The Circle of Willis is a circle of arteries around the brain. This loop leads to the potential for blood flow from both ends of the artery. Due to access issues, a balloon or coils are used to block off the far end of the artery while a ligature is used on the artery outside of the pouch. If the fungus is on a bone or non-arterial structure, it can be scraped off or treated with topical antifungals. Due to the risk of fatal hemorrhage, those options are not recommended for fungal infections involving an artery. Antifungal agents are not required if surgery is used, as the fungus cannot live without the arterial oxygen supply. Once the artery is occluded, the fungus dies off.
Bilateral infections are possible. Horner’s syndrome can develop due to involvement of the vagosympathetic trunk. The infections can also lead to dysphagia as the fungus affects nerve function to the tongue and swallowing muscles. Typically, horses with swallowing issues have a very poor prognosis.
Review Horner’s Syndrome clinical signs: ptosis, miosis, enophthalmos, patchy cervical swelling, nasal mucosa congestion.
Clinical signs – Bilateral epistaxis most common presentation. Epistaxis may be intermittent and may be copious. Dysphagia and/or Horner’s syndrome are possible.
Basilar skull fractures
Hemorrhage can develop in both guttural pouches with trauma to the back of the skull and/or the basisphenoid bones. This is most common in young horses that flip over backwards and land on the basilar skull region. This disorder can be difficult to differentiate from guttural pouch mycoses on initial presentation. Many of these horses will also have neurological symptoms and air may be seen mixed with the soft tissue blood opacity on radiographs. CT examination may be useful to fully evaluate the extent of damage. Prognosis is generally poor. There really aren’t surgical options. Consider this a differential.
Clinical signs- bilateral hemorrhagic nasal discharge and/or neurological dysfunction
Guttural pouch tympany 
Guttural pouch tympany is a non painful fluctuant swelling of one or both guttural pouches, particularly in Arab and German warmblood fillies. Air collects in the pouch as the opening operates as a one way valve rather than allowing bidirectional airflow. Respiratory distress is uncommon. Diagnosis is not difficult but it can be more challenging to determine if the disorder is unilateral or bilateral. On endoscopy, an abnormal guttural pouch opening is often evident. The opening to the guttural pouch is called the plica salpingopharyngeus. Medical treatment (NSAIDs) may resolve some cases. Surgery involves using a laser to create an opening either into the normal guttural pouch to allow air to exit the normal side or creating an opening into the pharynx. Prognosis is good if treated prior to the development of infection inside the pouch.
Clinical signs – nonpainful fluctuant swelling in the guttural pouch region
Temporohyoid osteopathy
Temporohyoid osteopathy (THO) is incompletely understood but involves proliferation of bone around the temporohyoid joint and can result in fusion of the joint between the stylohyoid bone and inner ear. With movement of the head or tongue, pain results and the stylohyoid bone can fracture. Remodeling of the joint and/or bone can be seen radiographically and endoscopically. The remodeling is suspected to result from local (inner ear) infection. Damage to local nerves can also result in poor tear production, dry eye and corneal ulcers. Surgical treatment involves cutting the ceratohyoid bone in the hyoid apparatus to relieve pressure on the joint and stylohyoid bone. Cutting the ceratohyoid bone is much easier and much less dramatic than cutting the stylohyoid bone and has the same result of disconnecting tongue and inner ear. Horses can be affected bilaterally. Prognosis depends upon the degree of dysfunction identified prior to surgery.
Clinical signs: corneal ulcers, conjunctivitis, dysphagia
Guttural pouch anatomy
Normal guttural pouch anatomy – see youtube video
Key Takeaways
Guttural pouches are expansions of the Eustachian tubes and disorders are found in horses but not in other domestic species (because they don’t have guttural pouches).
The most common disorders are related to strangles infections (empyema and chondroids), fungal infections (mycoses) and trapped air (tympany). Empyema and chondroids lead to purulent nasal discharge, fungal infections lead to potentially fatal hemorrhagic discharge and trapped air is found in Arab fillies and doesn’t bother them much (no impact on nasal discharge).
Resources
Anatomy of the Guttural Pouch, UGA free ibook
Treatment of guttural pouch mycosis with salpingopharyngostomy. Equine Vet Educ. 2023;35:585–587. short summary of many things guttural pouch
Guttural pouch disease causing neurological dysfunction, 2011 VCNA – table with really excellent explanation of nerves and side effects of guttural pouch disease
Update on disorders and treatment of the guttural pouch, VCNA: Equine Practice, April 2015, Vol.31(1), pp.63-89- explains how to drain chondroids surgically and goes into more detail about other procedures.
A diagnostic approach to congenital neck masses in foals. Equine vet. Educ. (2022) 34 (5) 231-234- good for weird differentials
Respiratory Disease Diagnostics in the Horse, VCNA: Equine Practice, August 2015, Vol.31(2), pp.307-336- medical and surgical diagnostics
Diagnosing guttural pouch disorders and managing guttural pouch empyema in horses, Vet Folio 2003 – need to register for student access
