15.7 Abortion
It is difficult to have a thorough discussion of baby making without a discussion of abortion. Few topics are more divisive than abortion, especially in countries such as the United States. The controversies surrounding abortion encompass legal, ethical, and moral issues that are beyond the scope of this text (and beyond the expertise of its authors). Thus, our discussion of abortion will be restricted to current abortion methods and then the legal standing of abortion in the United States. This information can help inform both one’s opinions on whether and under what conditions abortions should be legal and whether one considers an abortion a personally acceptable choice. However, this information alone cannot address the ethical and moral questions.
Abortion is defined as the termination of an established pregnancy. Somewhat confusingly, medical personnel sometimes refer to miscarriages (loss of a pregnancy by non-deliberate means) as “spontaneous abortions.” Abortions that are done to purposely end a pregnancy are sometimes called “induced abortions.” In this text when we use the term abortion we are referring to induced abortions.
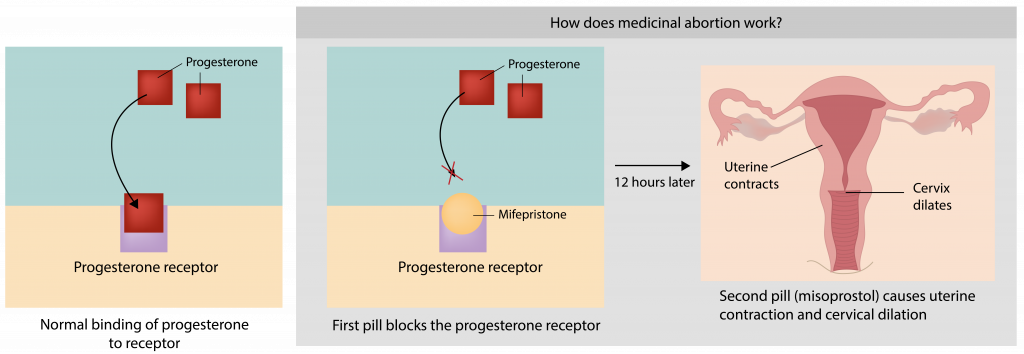
The vast majority (over 90%) of abortions occur in the first trimester. Abortions within the first trimester can be conducted by the administration of medicine or by physical extraction. Medicinal abortions are done in the U.S. until the 9th or 10th week of pregnancy. The most common medication for this purpose is a combination of pills commonly called RU486. One pill, mifepristone, functions by binding to progesterone receptors. As discussed earlier, progesterone is the hormone that maintains the lining of the uterus during a pregnancy. When the progesterone receptors are bound by this drug, progesterone cannot signal to maintain the uterine lining. The second drug, called misoprostol, causes the cervix to soften and the uterus to contract. Together these drugs cause the uterine lining to shed along with the implanted embryo.
An abortion by physical extraction involves either manual or drug-induced opening of the cervix and the placement of a small tube into the uterus. The tube suctions out the contents of the uterus with suction from a syringe or with a mechanical vacuum pump. Early term abortions that are overseen by qualified medical personnel are relatively safe for the pregnant person (that is, safer than carrying a pregnancy to term).
Second trimester abortions are much less common, and involve a more complicated procedure that involves the scraping of the lining of the uterus. Third trimester abortions are extremely rare and are often the result of life-threatening conditions to the pregnant individual, or discovery of fetal abnormalities that indicate the baby will not survive. The risks of abortion to the pregnant person increase with increasing stages of pregnancy.
In the United States prior to 1973, the legality of induced abortion was determined on a state-by-state basis. However, in 1973 the case of patient “Roe” went to the U.S. Supreme Court after she was denied an abortion in Texas. The lawyers for Roe argued that an abortion fell under medical privacy. The Supreme Court agreed, with the caveat that this right was balanced by the government’s interests in maternal health and potential human life. They determined that the state’s ability to interfere with pregnancy termination was influenced by fetal viability (the potential for the fetus to survive outside the uterus). However, the date at which a fetus is viable is somewhat of a moving metric, depending on medical advances, medical care available, and individual development.
In 2022, a case before the U.S. Supreme Court (Dobbs v. Mississippi Women’s Health Organization) challenged the constitutionality of a Mississippi ban on abortion after 15 weeks of gestation, the Court upheld the Mississippi abortion ban and overturned the 1973 Roe v. Wade decision, making it again the jurisdiction of individual states to determine the legality of abortion at any stage of pregnancy. Since this time abortion rights in many states have been dramatically curtailed or eliminated, and in other states the legal status of abortion has been in flux, as states individually grapple with their policy on abortion, either through the courts (determining if abortion rights are protected or curtailed by existing legislation or the state constitution) or through legislation that restricts abortion or establishes abortion rights.
As of the update of this material* abortion is banned in 14 states, restricted in 8 states, and legal until at least 22 weeks of pregnancy in 28 states. In states where abortion is banned, there are some exceptions in cases of rape, incest, or if the health of the pregnant person is in jeopardy. However, with severe penalties for doctors who perform abortions, and vagaries in the law about how likely an adverse health outcome would need to be to make the procedure qualify as an exception, many medical providers are not providing abortions that are necessary to protect the health of the pregnant person, nor are they performing procedures that resemble abortions such as the removal of unviable fetal tissue after a miscarriage, even when the health of the pregnant person is jeopardized. Since the implementation of these restrictions there have been several deaths of pregnant people that have been attributed to lack of, or delays in, medical care based on state abortion restrictions.
*This material was updated in September 2024. The authors have made their best effort to provide accurate information at this time, however there are many states that are in current flux about abortion rights, and the results of some ballot initiatives and court decisions may shift abortion access.
