9.2 Teenage Sex and Pregnancy
Learning Objectives
- Describe how many teenagers have had sex.
- List several problems associated with teenage pregnancy and birth.
- Discuss how to reduce teenage pregnancy and help teenage mothers.
We saw earlier that the percentage of teenagers who have sex greatly increased during the 1960s and 1970s. Regardless of what one thinks about premarital sex, this increase had at least two important practical consequences: It greatly increased the risk of teenage pregnancy, and it greatly increased the risk of getting HIV and other sexually transmitted diseases (STDs). For these and other reasons, teenage sex rightly arouses much concern. This section examines trends in teenage sex and pregnancy, the reasons for these trends, and possible measures for reducing teenage pregnancy. As part of this examination, it also discusses sexually transmitted disease, which affects sexually active teens but also sexually active people beyond their teen years.
Teenage Sexual Activity
As noted earlier, teenagers are much more sexually active today than they were before the sexual revolution. About 43 percent of never-married teens ages 15–19 of both sexes have had sexual intercourse (Martinez et al., 2011); this percentage represents a drop from its highest point, in 1988, of 51 percent for females and of 60 percent for males. About three-fourths of girls in today’s sexually experienced group and 85 percent of boys in this group use contraception, most often a condom, the first time they ever have sex. In their most recent act of sexual intercourse, almost 86 percent of girls and 93 percent of boys used contraception, again most often a condom.
The birth rate for females aged 15–19 in 2009 was 39.1 births per 1,000 females. This rate represented a substantial decline from the early 1990s, when the rate reached a peak of almost 60. However, it was still twice as high as Canada’s rate and much higher yet than other Western democracies (see Figure 9.4 “Teenage Birth Rates in Selected Western Democracies (Number of Annual Births per 1,000 Women Aged 15–19)”).
Figure 9.4 Teenage Birth Rates in Selected Western Democracies (Number of Annual Births per 1,000 Women Aged 15–19)
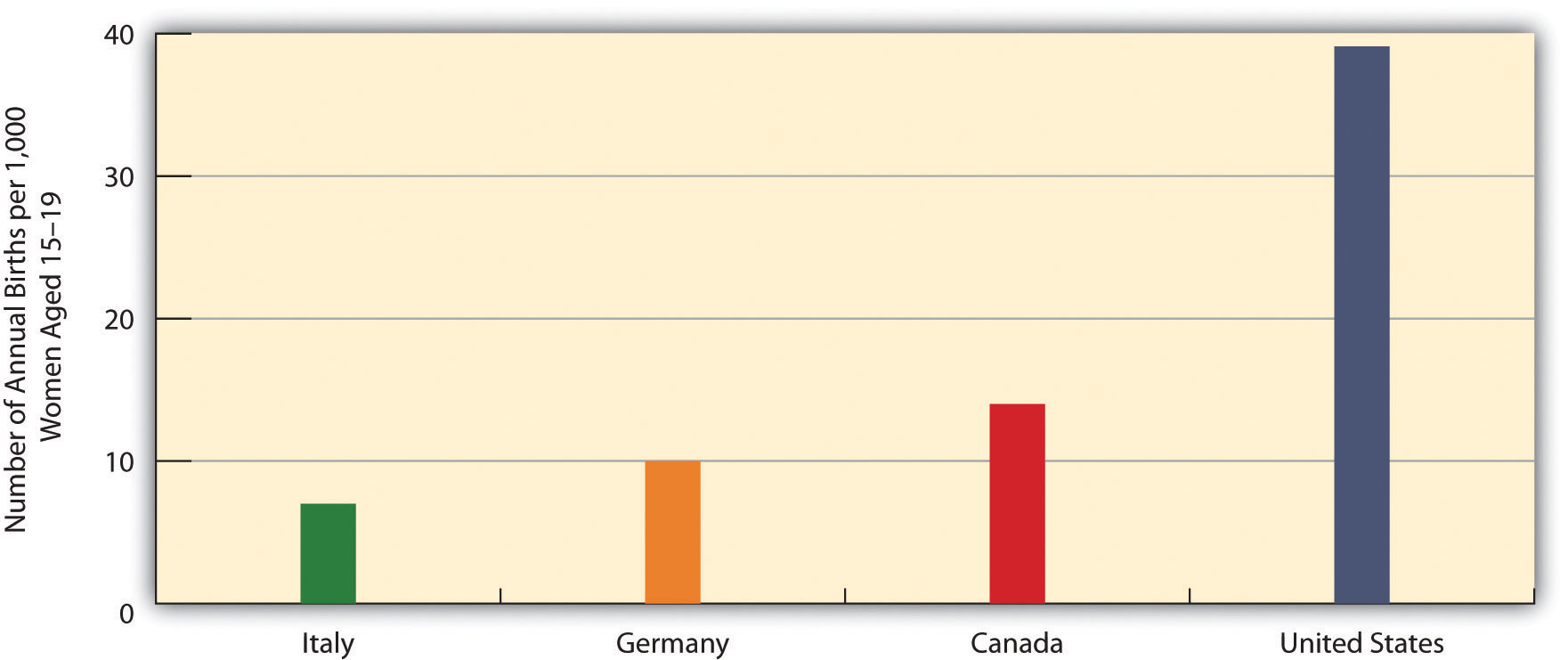
Source: Data from Martinez, G., Copen, C. E., & Abma, J. C. (2011). Teenagers in the United States: Sexual activity, contraceptive use, and childbearing, 2006–2010 national survey of family growth. Vital and Health Statistics, 23(31), 1–35.
If 43 percent of teens have had sexual intercourse, that means the majority of teens, 57 percent, have never had intercourse. It is interesting to examine their reasons for still being virgins. Table 9.4 “Main Reason Given for Never Having Sexual Intercourse, Ages 15–19 (%)” shows the relevant data. The top reason for both sexes is religion and morals, followed by concern about a possible pregnancy and not having found the right person with whom to have sex.
Table 9.4 Main Reason Given for Never Having Sexual Intercourse, Ages 15–19 (%)
| Females | Males | |
|---|---|---|
| Against religion or morals | 38 | 31 |
| Don’t want to get (a female) pregnant | 19 | 25 |
| Haven’t found the right person yet | 17 | 21 |
| Don’t want to get an STD | 7 | 10 |
| In a relationship, but waiting for the right time | 7 | 5 |
| Other reason | 12 | 8 |
Source: Martinez, G., Copen, C. E., & Abma, J. C. (2011). Teenagers in the United States: Sexual activity, contraceptive use, and childbearing, 2006–2010 national survey of family growth. Vital and Health Statistics, 23(31), 1–35.
The Problem of Teenage Pregnancy
Most teenage pregnancies and births are unplanned and are part of a more general problem for all women in their childbearing years. About one-half of all pregnancies in the United States, or more than 3 million pregnancies annually, are unplanned. Approximately 40 percent of these unplanned pregnancies end in abortion, and about 10 percent end by miscarriage. Putting all these numbers together, about 1.6 million live births happen each year as a result of unplanned pregnancies (National Campaign to Prevent Teen and Unplanned Pregnancy, 2011). The cost of medical services for unplanned pregnancies and for the infants that are born from many of them cost the nation more than $11 billion annually (Gold, 2011).
About one-fifth of all unplanned pregnancies, or almost 700,000 annually, occur to teenagers; another 50,000 teenage pregnancies are planned. These two figures add to 750,000 teenage pregnancies annually, with some 400,000 births resulting from these pregnancies (Kost, Henshaw, & Carlin, 2010). Altogether, about 18 percent of women, or one of every six females, become teen mothers, and in several southern and southwestern states this percentage is as high as 25–30 percent (Perper & Manlove, 2009).

About 18 percent of teenaged girls become mothers. In several southern and southwestern states, this percentage is as high as 25–30 percent.
bradfordst219 – CC BY 2.0.
Although teenaged pregnancies (and births from these pregnancies) are far from the majority of all pregnancies, unplanned or planned, they pose special problems (American College of Obstetricians and Gynecologists, 2011; Anderson, 2011). On the individual level, pregnant teenagers are more at risk than older pregnant women for high blood pressure and anemia, and they are also more likely to experience early labor, premature birth, and low birth weight. In addition, because teenagers are more likely than adults to have STDs, pregnant teenagers are more likely than older pregnant women to have an STD while they are pregnant, either because they already had an STD when they conceived or because they contract an STD from having sex during pregnancy.
Many pregnant teenagers decide to drop out of school. If they stay in school, they often must deal with the embarrassment of being pregnant, and the physical and emotional difficulties accompanying their teenage pregnancy can affect their school performance. Once the baby is born, child care typically becomes an enormous problem, whether or not the new mother is in school. Because pregnant teenagers disproportionately come from families that are poor or near poor, they have few financial resources and often have weak social support networks, either before or after the baby is born (Andrews & Moore, 2011).
At the societal level, teenage pregnancy and motherhood are very costly in at least two important respects. First, because pregnancy and childbirth complications are more common among teenagers, their health-care expenses during and after pregnancy and childbirth are often higher than the expenses incurred by older women. Medicaid, the federal government’s national health plan for poor families, often covers much of these expenses, and the premiums that private health insurance companies charge are higher than otherwise because of their expenses when they insure the families of pregnant teenagers.
Second, the children of teenage mothers are at risk for several kinds of behavioral and developmental problems. The Note 9.7 “Children and Our Future” box discusses these problems further.
Children and Our Future
Kids Having Kids: The Children of Teenage Mothers
Teenage mothers (ages 15–19) are often unprepared emotionally or practically to raise a child. They often have poor parenting skills and, for example, do not take the time to read daily to their children and otherwise stimulate their cognitive development. They are also less likely than older mothers to provide proper emotional support for their children. In addition, the stress they experience as very young mothers puts them at risk for neglecting or abusing their children. The fact that teenage mothers tend to come from low-income families and continue to live in poverty or near poverty after they become mothers compounds all these problems.
For all these reasons, the children of teenage mothers are at greater risk for several kinds of problems. These problems include impaired neurological development, behavioral problems, and poor school performance.
In particular, when compared to children born to older mothers, the children of teen mothers have lower cognitive scores on the average when they start kindergarten, and they continue to have lower math, reading, and vocabulary test scores as they grow older. These problems persist into their own adolescence, as they are less likely than children of older mothers to graduate from high school. Children of teen mothers are also somewhat more likely to have chronic health problems during childhood and adolescence. When the children of teenage mothers become adolescents, they are also more at risk for delinquency and drug use and to have a prison record by the time they reach young adulthood.
The teenage pregnancy and birth rates in the United States are by far the highest of all Western democracies. The problems that children of teen mothers experience underscore the need for our nation to do everything possible to prevent teenage pregnancy.
Sources: Andrews & Moore, 2011; Hoffman & Maynard, 2008
Trends in Teenage Pregnancy
The bad news is that there are far too many teenage pregnancies. The good news is that the rate of teenage pregnancy has declined rather dramatically since the early 1990s.
The teenage pregnancy rate is commonly expressed as the annual number of pregnancies per 1,000 women aged 15–19. In 2006, this rate was 71.5, equal to 7.15 percent of all women in this age bracket (Kost et al., 2010). Because many women in this age group either have never had sex or have not had sex in the past year, it is instructive to consider the pregnancy rate among women ages 15–19 who are sexually active. In 2006, this rate was 152.8 per 1,000, equal to 15.28 percent of all sexually active women in this age group.
As high as these rates are, and they are much higher than the rates in other Western democracies, the US teenage pregnancy rate is much lower now than it was in the early 1990s. Figure 9.5 “Pregnancy Rates for US Women Aged 15–19, 1972–2006 (Number of Pregnancies per 1,000 Women Aged 15–19)” displays this dramatic trend. Teenage pregnancy reached a peak rate of 116.9 in 1990 before falling rather steadily to its 2006 rate of 71.5, a much lower rate than existed during the early 1970s. Reflecting the decline in teenage pregnancy, teenage births, as noted earlier, also reached a record low of 39.1 births per 1,000 women ages 15–19 in 2009, as compared to its peak rate of 61.8 in 1991. Despite this dramatic decline, the US teenage birth rate remains the highest of all Western democracies. Experts attribute the decline in teenage pregnancy and birth mostly to increased contraceptive use (stemming from a combination of increased sex education in the schools and increased provision of contraceptives to teenagers) and, to a smaller extent, to reduced sexual activity among some teenagers (Kost et al., 2010).
Figure 9.5 Pregnancy Rates for US Women Aged 15–19, 1972–2006 (Number of Pregnancies per 1,000 Women Aged 15–19)
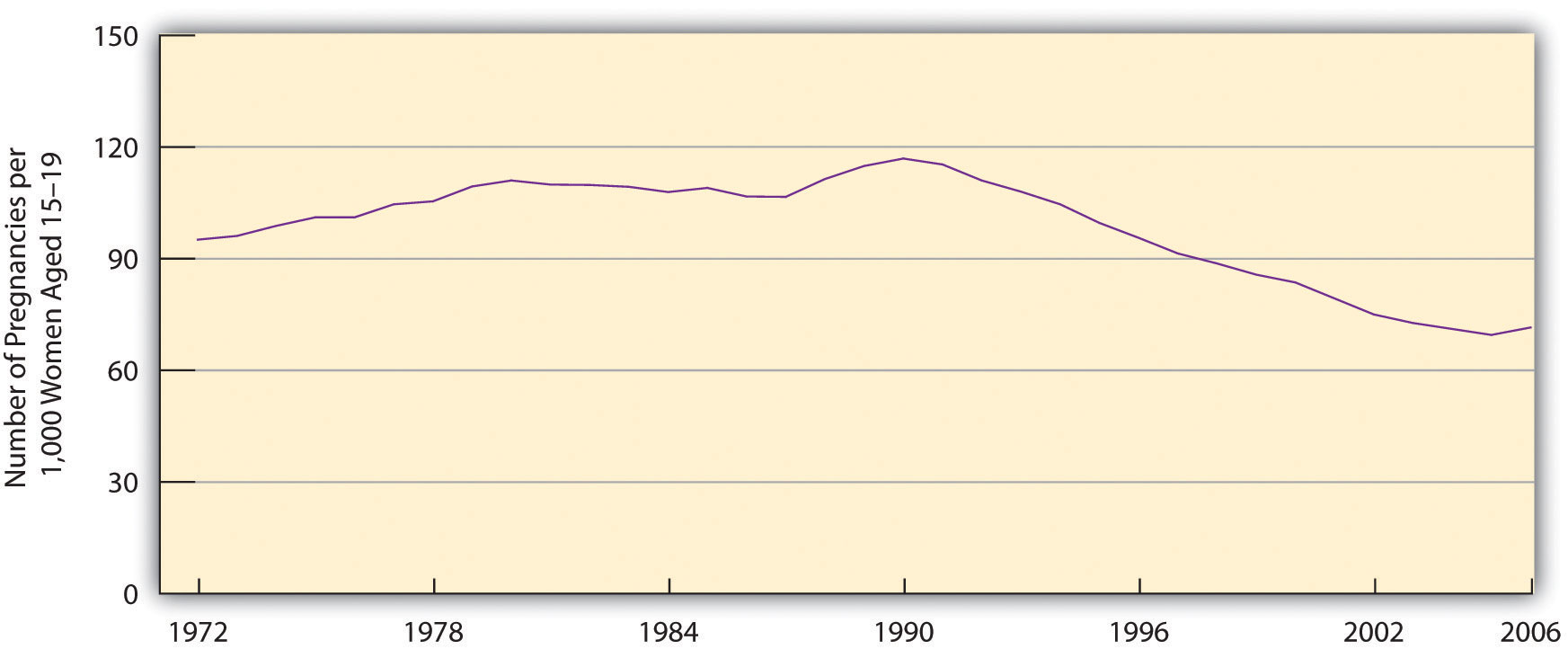
Source: Data from Kost, K., Henshaw, S., & Carlin, L. (2010). US teenage pregnancies, births and abortions: National and state trends and trends by race and ethnicity, 2010. New York, NY: Guttmacher Institute.
Correlates of Teenage Pregnancy
We have already noted that teenagers from poor or near-poor families are at greater risk for becoming pregnant. In addition to social class, two other important correlates of teenage pregnancy are race/ethnicity and geography.
Figure 9.6 “Race/Ethnicity and Teenage Pregnancy, 2006 (Number of Pregnancies per 1,000 Women Aged 15–19)” displays the racial/ethnic differences for teenage pregnancy, which are rather large. The pregnancy rates for black and Hispanic teenagers are almost three times greater than the rates for non-Hispanic whites.
Figure 9.6 Race/Ethnicity and Teenage Pregnancy, 2006 (Number of Pregnancies per 1,000 Women Aged 15–19)
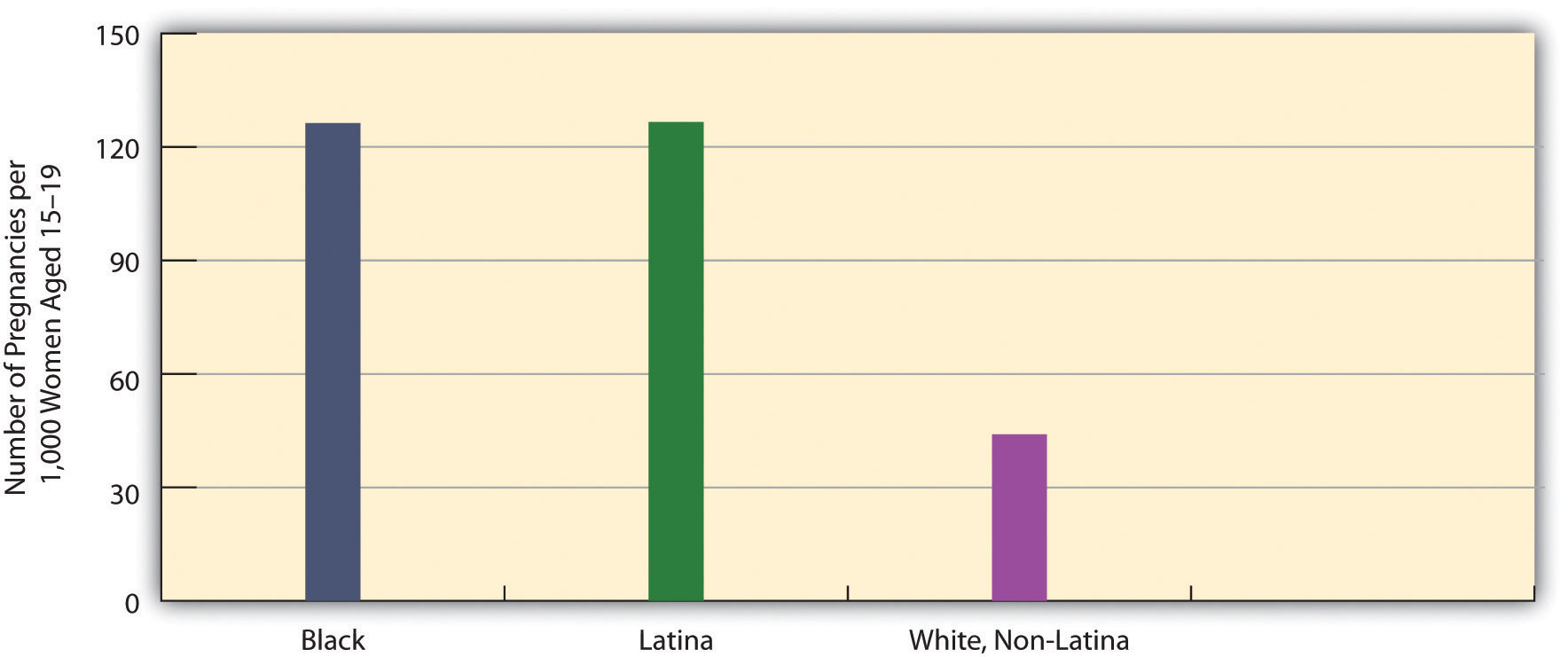
Source: Data from Kost, K., Henshaw, S., & Carlin, L. (2010). US teenage pregnancies, births and abortions: National and state trends and trends by race and ethnicity, 2010. New York, NY: Guttmacher Institute.
Large differences also exist in teenage pregnancy rates by state and the regions of the country into which the states fall. In general, the South has a higher teenage pregnancy rate than the rest of the nation (see Figure 9.7 “Teenage Pregnancy Rates in the United States, 2005 (Number of Pregnancies per 1,000 Women Aged 15–19)”), although there are individual differences by state. The South’s generally higher rate stems largely from its higher poverty rate and racial/ethnic composition. As the opening news story on Texas indicates, sex education programs emphasizing safe sex are also less common in Southern states than in many other states. The same difference holds for the provision of contraceptives by Planned Parenthood and other agencies and organizations. The lack of these two important pregnancy-prevention measures probably also contributes to the South’s higher teenage pregnancy rate.
Figure 9.7 Teenage Pregnancy Rates in the United States, 2005 (Number of Pregnancies per 1,000 Women Aged 15–19)
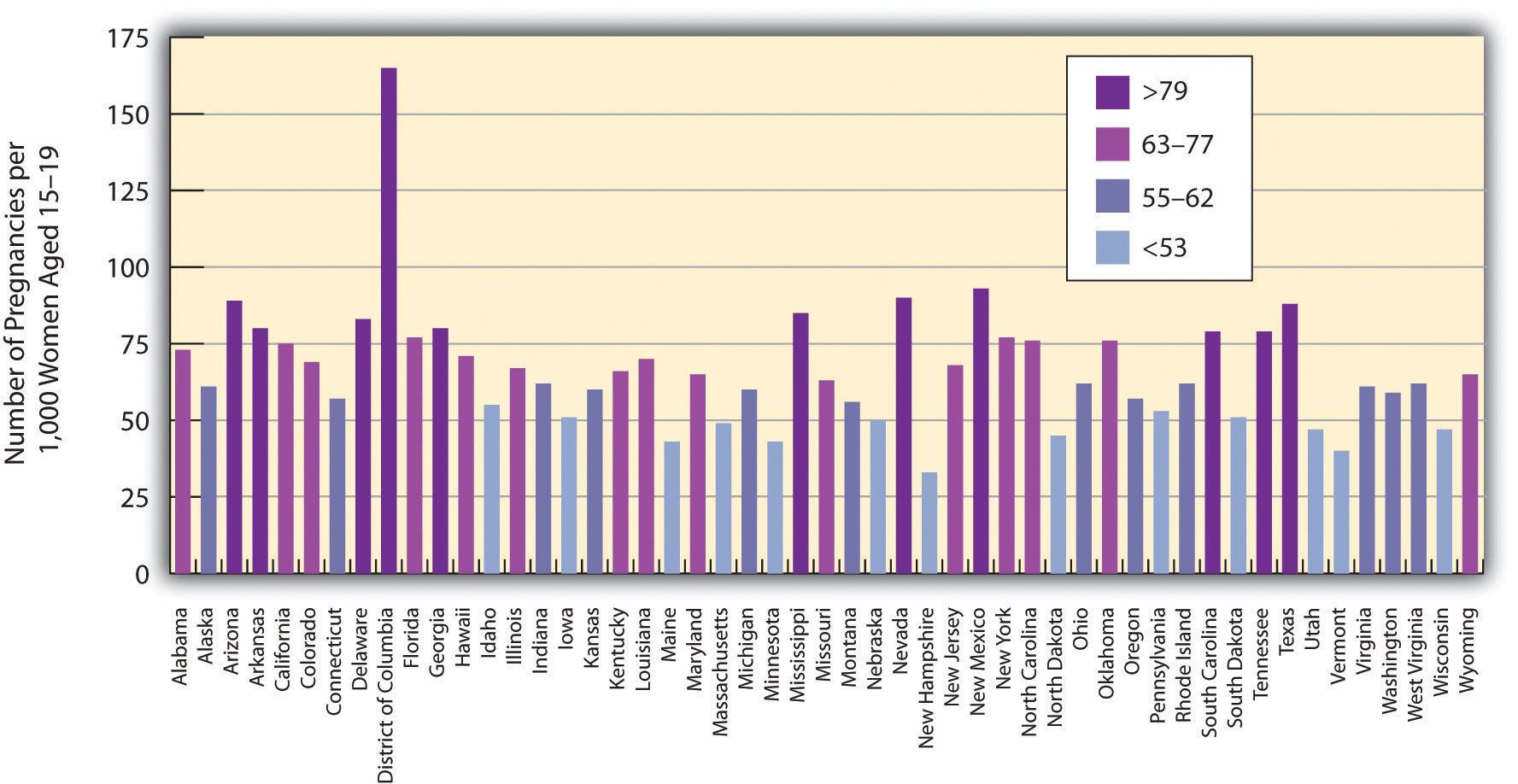
Source: Data from Kost, K., Henshaw, S., & Carlin, L. (2010). US teenage pregnancies, births and abortions: National and state trends and trends by race and ethnicity, 2010. New York, NY: Guttmacher Institute.
Sexually Transmitted Diseases
In addition to pregnancy and birth, another problem associated with teenage sexual activity is the transmission of sexually transmitted diseases (STDs). This is a problem during the teenage years, but it is even more of a problem during young adulthood, when sexual activity is greater than during adolescence (Wildsmith, Schelar, Peterson, & Manlove, 2010). The STD rate in the United States is higher than in most other Western democracies. Almost 19 million new cases of STDs are diagnosed annually, and more than 65 million Americans have an incurable STD such as herpes. Although teens and young adults ages 15–24 compose only one-fourth of sexually active people, they account for one-half of all new STDs. Despite this fact, most young adults who test positive for an STD did not believe they were at risk for getting an STD (Wildsmith et al., 2010).

Teens and young adults ages 15–24 compose one-fourth of all sexually active people, but they account for one-half of new sexually transmitted diseases.
Brian Rosner – New Friends at CU – CC BY 2.0.
In any one year, 15 percent of young adults ages 18 and 26 have an STD. This figure masks a significant gender difference: 20 percent of young women have had an STD in the past year, compared to 10 percent of young men. It also masks important racial/ethnic differences: 34 percent of young African Americans have had an STD in the past year, compared to 10 percent of Asians, 15 percent of Hispanics, and 10 percent of whites.
Three types of sexual behaviors increase the risk of transmitting or contracting an STD: having sex with at least three partners during the past year, having a sex partner with a known STD, and not using a condom regularly. About 17 percent of sexually active young adults have had at least three partners during the past year, and 8 percent have had a partner with a known STD. Three-fourths of unmarried sexually active young adults do not use a condom regularly. Combining all these risk factors, 39 percent have engaged in one risk factor in the past year, 14 percent have engaged in at least two risk factors, and the remainder, 48 percent, have engaged in no risk factors (Wildsmith et al., 2010).
Reducing Teenage Pregnancy and Helping Teenage Mothers
Teenage pregnancies cannot occur in either of these two situations: (1) Teenagers do not have sex, or (2) they use effective contraception if they do have sex. If we could wave a magic wand or turn the clock back to before the 1960s, it might be possible to greatly reduce the number of teenagers who have sex, but that day is long past. Teenage sex increased during the 1960s and 1970s and, despite some slight declines after HIV and AIDS became a worldwide problem during the 1980s and 1990s, remains much more frequent than before the sexual revolution. Most sexual behavior researchers believe that pleas for abstinence, as well as sex education programs that focus solely or almost entirely on abstinence, do not help to reduce teen sex and pregnancy (Ball & Moore, 2008).
If this is true, they say, then the best strategy is to use a harm reduction approach. We first encountered this term in Chapter 7 “Alcohol and Other Drugs”’s discussion of illegal drugs. A harm reduction approach recognizes that because certain types of harmful behavior are inevitable, our society should do its best to minimize the various kinds of harm that these various behaviors generate. In regard to teenage sex and pregnancy, a harm reduction approach has two goals: (1) to help reduce the risk for pregnancy among sexually active teens and (2) to help teenage mothers and their children.
Reducing Pregnancy
To achieve the first goal, parents, sex education classes, family planning clinics, youth development programs, and other parties must continue to emphasize the importance of waiting to have sex but also the need for teenagers to use contraception if they are sexually active. In addition, effective contraception (birth control pills, other hormonal control, and also condoms, which protect against STDs) must be made available for teenagers at little or no cost. Studies indicate that these two contraception strategies do not lead to more teenage sex, and they also indicate that consistent contraceptive use greatly reduces the risk of teenage pregnancy. As one writer has summarized these studies’ conclusions, “Contraceptives no more cause sex than umbrellas cause rain…When contraception is unavailable, the likely consequences is not less sex, but more pregnancy” (Kristof, 2011, p. A31).
People Making a Difference
Helping Teenagers Reduce the Risk of Pregnancy
The Metro Council for Teen Potential (MCTP) is a membership coalition in Rochester, New York, that “promotes a comprehensive community-wide approach to foster youth assets and youth health,” according to its website. To do so, MCTP provides various kinds of information to its member agencies and organizations, including the latest data on pregnancy and other problems facing teens and the latest information on the “best practices” to use to help teens. It has also developed a youth curriculum and media campaign aimed at informing youths about risky behaviors, sexuality, and other aspects of their lives. Its member groups include the Rochester School District and youth development organizations throughout Rochester.
An important focus of MCTP’s efforts is teen pregnancy, and MCTP has received substantial funding from the US Centers for Disease Control and Prevention to formulate and implement strategies to prevent teen pregnancies. Its website includes results from a random survey of Rochester-area teens about their sexual behavior, views about teen pregnancy, substance use, and other behaviors and attitudes. The website also includes some basic data on Rochester teens’ sexual experiences. For example, the 2006 teen birth rate in Rochester was 76 births per 1,000 girls ages 15–19; this rate was much higher than the US rate of 42 and the New York state rate of 26.
MCTP supports several initiatives in Rochester that focus on teenage sexuality and pregnancy. One set of programs called CONECTS provides a variety of teenage pregnancy prevention strategies through such subcontractors as the YWCA. Another program, In-Control, provides reproductive health care and education through Planned Parenthood. A third program, Family Talk, involves workshops that aim to help parents of teens talk more effectively with their children about sexuality and substance abuse.
For these and other efforts, MCTP has won the Organizational Award from the Youth Services Quality Council for the high quality of its work for youths and their families. In helping to reduce teen pregnancy and address other problems facing teenagers in Rochester, the Metro Council for Teen Potential is making a difference. For further information, visit its website at http://www.metrocouncil.us.
In this regard, a recent report of the Guttmacher Institute called contraception a “proven, cost-effective strategy” (Gold, 2011, p. 7). It added, “Contraception is almost universally accepted as a way to reduce the risk of unintended pregnancy…Contraceptive use reduces the risk of unintended pregnancy significantly, and consistent contraceptive use virtually eliminates it.” The report noted that government-funded family planning agencies prevent 2 million unintended pregnancies annually by providing contraception to 9 million young and low-income women each year. Because most of the women who would have these prevented pregnancies would be eligible for Medicaid, the Medicaid savings from these prevented pregnancies amount to about $7 billion annually. An expansion of family planning services would almost certainly be an effective strategy for reducing teenage pregnancies as well as unplanned pregnancies among older women.
Another strategy to prevent teenage pregnancy involves the use of early childhood intervention (ECI) programs. Many such programs exist, but they generally involve visits by social workers, nurses, and other professionals to the homes of children who are at risk for neurological, emotional, and/or behavioral problems during their first several years and also as they grow into adolescents and young adults (Kahn & Moore, 2010). It might sound like a stereotype, but these children are disproportionately born to single, teenage mothers and/or to slightly older parents who live in poverty or near poverty. Long-term evaluation studies show that the best of these programs reduce the likelihood that the very young children they help will become pregnant or have children of their own after they become teenagers (Ball & Moore, 2008). In effect, helping young children today helps prevent teenage pregnancy tomorrow.
Helping Teen Mothers
Because teen pregnancies occur despite the best prevention efforts, the second goal of a harm reduction approach is to help teens during their pregnancy and after childbirth. This strategy has the immediate aim of providing practical and emotional support for these very young mothers; it also has the longer-term aims of reducing repeat pregnancies and births and of preventing developmental and behavior problems among their children.
To achieve these aims, ECI programs have again been shown to be helpful (Ball & Moore, 2008). Another type of program to help teen mothers involves the use of second-chance homes, which are maternity group homes for unmarried teen mothers (Andrews & Moore, 2011). One of the many sad facts of teenage motherhood is that teen mothers often have nowhere to live. A teen mother’s parent(s) may refuse to let her and her infant live with them, either because they are angry at her pregnancy or because they simply do not have the room or financial means to house and take care of a baby. Or a pregnant teen may decide to leave her parents’ home because of the parents’ anger or because they refuse to let her continue seeing the child’s father. In another possibility, a teen mother may begin living with the father, but these unions are typically unstable and often end, again leaving her and her child without a home. As well, many teen mothers were runaways from home before they became pregnant or were living in foster care. Because of all these situations, many teen mothers find themselves without a place to live.

Second-chance homes provide many kinds of services for pregnant teenagers and teen mothers, many of whom are unable to continue living with their own parents.
Teresa Rodríguez – cynthea y kabeer jr – CC BY-ND 2.0.
In second-chance homes (which, depending on the program, are in reality one large house, a set of apartments, or a network of houses), mothers and children (as well as pregnant teens) receive shelter and food, but they also receive important services, such as childrearing help, educational and vocational counseling and training, family planning counseling, and parenting classes. Although rigorous evaluation studies do not yet exist of the effectiveness of second-chance homes, they do seem to offer a valuable resource for teen mothers and their children (Andrews & Moore, 2011).
Addressing Poverty
A final strategy for addressing the problem of teenage sex and pregnancy is to address a more general societal condition that helps produce teenage sex and pregnancy. This condition is poverty. As noted earlier, children who grow up in poor families and in disadvantaged neighborhoods—those with high rates of poverty, unemployment, high school dropouts, and so forth—are more likely to have sex earlier as teens and to become pregnant (Harding, 2003; Scott, Steward-Streng, Barry, & Manlove, 2011). Efforts that reduce poverty (see Chapter 2 “Poverty”) and improve the conditions of disadvantaged neighborhoods will also reduce the collateral effects of poverty, including teenage pregnancy.
Key Takeaways
- The United States has the highest rates of teenage pregnancy and birth of all Western democracies. However, these rates have declined substantially from the early 1990s.
- Pregnancies and births among teenagers incur higher health-care costs than those among older women. In addition, children of teenage mothers are at risk for several kinds of developmental, cognitive, and behavioral problems.
- A key strategy to reduce teenage pregnancies involves the provision and use of effective contraception at little or no cost. A key strategy to help teen mothers and their children involves second-chance homes and early childhood intervention programs.
For Your Review
- Imagine that you became a parent at age 17. How would your life have been different from what it is now?
- Many sexually active teenagers do not use contraception regularly. Why do you think they do not use it more often?
