7.2 Drugs and Drug Use Today
Learning Objectives
- Summarize the different types of drugs.
- Explain the various harms caused by alcohol and tobacco.
- Understand the effects of marijuana, cocaine, and other illegal drugs.
A drug may be defined as any substance other than food that, when taken into the body, affects the structure and/or functioning of the body. Defined this way, many common substances contain drugs or are drugs: coffee, No-Doz, and other products to keep us alert; aspirin, acetaminophen, ibuprofen, and other pain relievers; Tums, Rolaids, and other products that reduce heartburn; Metamucil and other products that reduce constipation; Robitussin, Sudafed, and other cold medicines; and so forth. If you have ever used one of these products, you are technically a drug user, however silly that might sound.
Many prescription drugs also certainly exist: Prozac and other antidepressants; Valium and other tranquilizers; Lipitor and other cholesterol drugs; Yasmin, Yaz and other birth control pills; Viagra and other products that relieve erectile dysfunction; and so forth. Sales of these prescription drugs amount to tens of billions of dollars annually.
The following substances are also drugs: alcohol, ecstasy, cocaine, heroin, marijuana, LSD, methamphetamine, PCP, and tobacco. Much has been written about these drugs, and we will discuss them further later in this section. But note that two of these drugs, alcohol and tobacco, are legal after a certain age, while the remaining drugs are illegal.
One of the problems in deciding how to think about and deal with drugs is that this distinction between legal drugs and illegal drugs has no logical basis. It makes sense to assume that the illegal drugs should be the ones that are the most dangerous and cause the most physical and social harm, but that is not true. Rather, alcohol and tobacco cause the most harm even though they are legal. As Kleiman et al. (2011, p. xviii) note about alcohol, “When we read that one in twelve adults suffers from a substance abuse disorder or that 8 million children are living with an addicted parent, it is important to remember that alcohol abuse drives those numbers to a much greater extent than does dependence on illegal drugs.” Tobacco kills about 435,000 Americans annually by causing premature death, and alcohol kills about 85,000 annually through its effects on the liver and other body organs (Mokdad, Marks, Stroup, & Gerberding, 2004).
Putting these numbers together, some 520,000 Americans die annually from alcohol and tobacco use. Meanwhile, the physiological effects of all illegal drugs combined kill an estimated 17,000 Americans annually (Mokdad et al., 2004), a number that is only just above the number of annual deaths (16,500) from nonsteroidal inflammatory drugs (NSAIDs) such as aspirin and ibuprofen (Frech & Go, 2009). Figure 7.1 “Annual Deaths from Legal and Illegal Drugs” depicts the huge difference between deaths from alcohol and tobacco as legal drugs and from illegal drugs.
Figure 7.1 Annual Deaths from Legal and Illegal Drugs
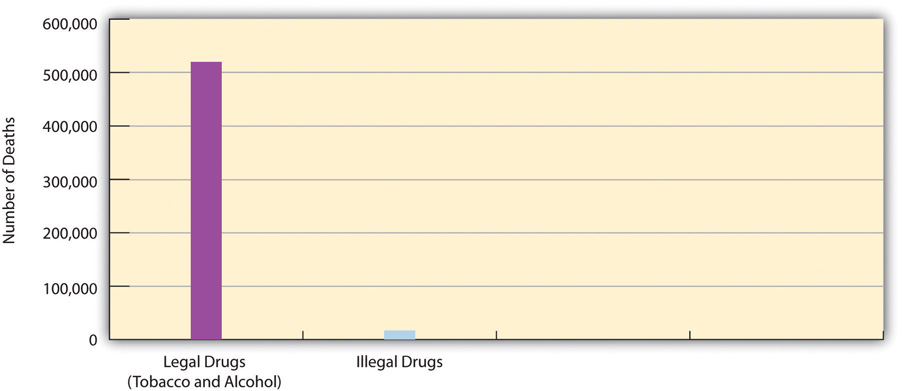
Source: Mokdad, A. H., Marks, J. S., Stroup, D. F., & Gerberding, J. L. (2004). Actual causes of death in the United States, 2000. Journal of the American Medical Association, 291(10), 1238–1245.
We return to the issue of the relative harm of legal and illegal drugs toward the end of the chapter when we discuss drug policy. In the meantime, keep in mind two related facts: (1) all drugs can be dangerous, and (2) some drugs are much more dangerous than others. Two aspirins are safe to take, but a bottle of aspirin can kill someone. Two cups of coffee a day are fine, but drinking many cups a day can cause anxiety, insomnia, and headaches. One drink of alcohol is safe to take, but several drinks in a short time amount to binge drinking, and long-term use of alcohol can kill someone. One snort of cocaine is usually safe, but even one snort can result in a sudden fatal heart attack, and long-term use often has serious health consequences.
Types of Drugs
Drugs are commonly classified into certain categories according to their physiological effects. All drugs may make us feel good, but they do so in different ways. Because some drugs are much more potent than other drugs, there is much variation within each category. Partly because many drugs have multiple effects, many different classifications of drugs exist. A common classification includes the following categories: depressants, hallucinogens, marijuana, narcotics, and stimulants.
Depressants
Depressants slow down the activity of the central nervous system. Depending on the specific drug, they help induce drowsiness and relaxation, and they can reduce anxiety and pain. Several types of depressants exist. Analgesics reduce pain and include over-the-counter products such as aspirin, acetaminophen (the major ingredient in Tylenol), and ibuprofen (the major ingredient in Advil and Motrin), and many prescription medicines that contain acetaminophen. Sedatives help people relax and include alcohol, barbiturates, and sleep medicines such as Sominex and Tylenol PM (both over-the-counter) and Ambien and Valium (both prescription). Large doses of depressants may lead to physical dependence and sometimes death.
Hallucinogens
Hallucinogens are mind-altering drugs that cause delusions or hallucinations. Their ranks include ecstasy, LSD, mescaline, and PCP. Many people who use a hallucinogen report that the mind-altering effects of the drug provide them a truly wonderful experience, but many also find the effects to be troubling at best and horrible and terrifying at worst. Long-term effects include hallucinations that occur without any drug use preceding them.
Marijuana
Marijuana is by far the most popular illegal drug in the United States.
Modern Scribe Photography – Maryjane 4-20-2010 (420) – CC BY-ND 2.0.
Because marijuana’s effects do not fit neatly into any other category of drug, marijuana (along with its close cousin, hashish) is often considered to be its own category. As we will see later, it is by far the most popular illegal drug in the United States. Its effects include distortion of time and space, euphoria, hunger, increased sensory perception, and relaxation.
Narcotics
Narcotics are sometimes classified under depressants because they slow down the central nervous system, but they are often still considered as their own category. They are highly effective at relieving pain and are a common substance in prescription medicines for severe pain. By definition, all narcotics are derived from opium, either in its natural form or in a synthesized form. Examples of narcotics include codeine, heroin, methadone, and morphine. In addition to relieving pain, narcotics may induce drowsiness, euphoria, and relaxation. Although narcotics do not damage bodily organs, they are very physically addictive, and high doses can be fatal.
Stimulants
Stimulants have the opposite effect of depressants by speeding up the central nervous system. They increase alertness and energy and can produce euphoria or anxiety. Some are legal and some are illegal, and many very different drugs are all considered stimulants: caffeine, cocaine, methamphetamine and other amphetamines, nicotine (tobacco), and Ritalin. Stimulants can be very physically addictive, and nicotine is thought to be more addictive than heroin. While caffeine is very safe as long as someone does not have too many cups of coffee daily, many other stimulants may have dangerous short-term or long-term side effects on the cardiovascular system.
Not all drugs can be discussed in one chapter. In choosing which drugs to discuss in a book on social problems, it makes sense to discuss the drugs that probably concern Americans the most. We thus focus in the remainder of this section mostly on alcohol, tobacco, marijuana, cocaine, and heroin.
Legal Drugs
As noted earlier, alcohol and tobacco (nicotine) are two legal drugs that are very common and that together kill hundreds of thousands of Americans annually. According to national survey evidence collected by the Substance Abuse and Mental Health Services Administration (SAMHSA) of the federal government, most people 12 and older (as well as many younger than 18) have tried alcohol, and over half the public drinks currently (defined as having had at least one drink in the past month). While many people have tried tobacco, only slightly more than one-fourth of the public uses it currently (at least once during the past month). Table 7.1 “Prevalence of Alcohol and Tobacco Use, Ages 12 and Older, 2010*” summarizes the prevalence of alcohol and nicotine use. Translating some of these percentages into actual numbers, almost 70 million Americans are current tobacco users (mostly by smoking cigarettes), and 131 million are current alcohol users.
Table 7.1 Prevalence of Alcohol and Tobacco Use, Ages 12 and Older, 2010*
| Lifetime | Past year | Past month | |
|---|---|---|---|
| Alcohol | 82.5 | 66.4 | 51.8 |
| Tobacco | 68.7 | 32.8 | 27.4 |
| * Percentage using in designated time period | |||
Source: Substance Abuse and Mental Health Services Administration. (2011). Results from the 2010 national survey on drug use and health: Summary of national findings. Rockville, MD: Author.
With this backdrop, we now discuss these two legal but very harmful drugs in greater detail.
Alcohol
Moderate alcohol use (more than one drink per day for an adult female and two drinks per day for an adult male) is relatively safe for most people and may even have health benefits (Harvard School of Public Health, 2012). The problem is that many people drink much more than moderately. As the Harvard School of Public Health (2012) explains, “If all drinkers limited themselves to a single drink a day, we probably wouldn’t need as many cardiologists, liver specialists, mental health professionals, and substance abuse counselors. But not everyone who likes to drink alcohol stops at just one. While most people drink in moderation, some don’t.”
SAMHSA survey data show the extent of such problem drinking, as its survey measures both binge drinking (five or more drinks on the same occasion—within two hours of each other—on at least one day in the past month) and heavy drinking (binge drinking on at least five days in the past month). Table 7.2 “Prevalence of Binge and Heavy Alcohol Use, 2010*” presents the relevant data for people 12 and older and also for those aged 18–20, the customary age for people in their first two years of college.
Table 7.2 Prevalence of Binge and Heavy Alcohol Use, 2010*
| Ages 12 and older | Ages 18–20 | |
|---|---|---|
| Binge use | 23.1 | 33.3 |
| Heavy use | 6.7 | 11.3 |
| * Percentage engaging in alcohol use | ||
Source: Substance Abuse and Mental Health Services Administration. (2011). Results from the 2010 national survey on drug use and health: Summary of national findings. Rockville, MD: Author.
As Table 7.2 “Prevalence of Binge and Heavy Alcohol Use, 2010*” indicates, almost one-fourth of all people 12 and older and one-third of those aged 18–20 engage in binge drinking, while almost 7 percent and about 11 percent, respectively, engage in heavy drinking. The figures for those 12 and older translate to almost 59 million binge drinkers and 17 million heavy drinkers. These numbers show that tens of millions of people abuse alcohol annually and underscore the problem of dealing with problem drinking.
The amount of alcohol consumed annually by occasional, moderate, and heavy drinkers is staggering. The relevant data appear in Table 7.3 “Alcohol Consumption in the United States, 2010”. Americans drink 7.6 billion gallons of alcohol annually, equivalent to 126 billion standard drinks. This number of drinks works out to 496 drinks per person annually for the 12 and older population and 748 drinks per person for the 12 and older population that drinks at all. Keep in mind that this is just an average. The heavy drinkers identified in Table 7.2 “Prevalence of Binge and Heavy Alcohol Use, 2010*” have many more than 748 drinks every year, while light drinkers have only a relative handful of drinks.
Table 7.3 Alcohol Consumption in the United States, 2010
| Number of gallons | Equivalent number of standard drinks* | |
|---|---|---|
| Beer | 6.4 billion | 68.2 billion |
| Wine | 713.2 million | 18.3 billion |
| Spirits | 463.1 million | 39.5 billion |
| Total | 7.6 billion | 126.0 billion |
| * one drink = 12 ounces of beer, 5 ounces of wine, or 1.5 ounces of spirits | ||
Source: Beer Institute. (2011). Brewers almanac, 2011. Washington, DC: Author.
The Drinking Culture and the Alcohol Industry
As noted earlier, alcohol has a long history in the United States and an even longer history in much of the rest of the world. When we think about the tens of millions of Americans who drink at least occasionally, the ads for beer and wine and hard liquor that appear regularly in the popular media, and the thousands of bars and related venues across the country, it is certainly no exaggeration to say that we have a drinking culture.
Once upon a time, the federal and state governments tried to eliminate this culture. We are speaking, of course, about Prohibition. The passage of the Eighteenth Amendment to the US Constitution in January 1919 banned the manufacture, sale, and transportation of alcohol; the ban took effect a year later. For reasons we will discuss later, the ban was eventually deemed a failure, and the passage of the Twenty-First Amendment in 1933 repealed the Eighteenth Amendment. The manufacture, sale, and transportation of alcohol became legal once again.
Alcohol manufacturing and sales are a major industry worldwide today. Several alcohol companies rank among the largest corporations in the world as well as in the United States (Jernigan, 2009). US alcohol sales amount to about $160 billion annually, and they rose by 20 percent in the 2010–2011 period during the faltering economy (Smith, 2011). The amount of money the public spends on alcohol equals 12.5 percent of what it spends on food (US Department of Agriculture, 2011). The alcohol industry provides about 2 million jobs annually, more than $40 billion in wages, and more than $50 billion in taxes, and it contributes more than $160 billion to the annual national economy (Distilled Spirits Council of the United States, 2011). All these figures show that the alcohol industry plays a significant role in the US economy.
Despite this role, if the United States does indeed have a drinking culture, the alcohol industry bears a major share of the responsibility. As the American Medical Association (2004) has stated,
Like the tobacco industry, the alcohol industry produces a legal, widely consumed drug; is dominated by relatively few producers; and utilizes a powerful combination of advertising dollars, savvy marketing, political campaign contributions, and sophisticated lobbying tactics to create and maintain an environment favorable to its economic and political interests. It requires the recruitment of new, youthful drinkers to maintain and build its customer base…As a chemical that affects our bodies, alcohol is a powerful drug resulting in more premature deaths and illnesses than all illicit drugs combined. Yet the industry has shaped public opinion and forced government to treat it not as a drug but as a cultural artifact, a valued legal commodity, almost a food, even a necessity of life.
As just one example of how the alcohol industry promotes its “powerful drug,” the headline of a recent news article declared that the “alcohol companies go online to lure young drinkers” (Gardner, 2010). According to the report, alcohol companies are increasingly using Facebook and other social media to persuade young people to buy and drink their products. Not surprisingly, many of these young targets turn out to be under the legal drinking age of 21 because they are easily able to gain access to alcohol sites. This problem led a public health professor to observe, “Close to 5,000 people under the age of 21 die of alcohol overuse each year. Virtual worlds show all of the appeal and none of the consequences of alcohol use and undercut efforts to reduce the incidence of underage drinking. At this point, alcohol companies appear limited only by their imaginations and pocketbooks” (Gardner, 2010).

The alcohol industry is a major part of the US and worldwide economies and provides about 2 million jobs annually in the United States.
amateur photography by michel – Aardwolf Brewing Company – CC BY 2.0.
Consequences of Alcohol Abuse
Despite alcohol’s immense popularity, the fact remains that more than 18 million Americans abuse it (Harvard School of Public Health, 2012). This heavy rate of abuse means that alcohol has serious personal and social consequences. One set of consequences involves personal health. We noted earlier that alcohol abuse is responsible for about 85,000 deaths annually through the physiological damage it does. Heavy alcohol use can destroy the liver, increase blood pressure, weaken the heart and immune system, and cause sexual dysfunction. It can lead to neurological problems and also raises the risk of incurring several kinds of cancer. Binge drinking can cause serious immediate health problems because it may lead to someone overdosing on alcohol. About 800,000 adults are hospitalized every year for alcohol overdoses, and tens of thousands more are hospitalized because they have consumed alcohol along with prescription narcotic pain medications, a combination that can be deadly (National Institutes of Health, 2011).
In addition to these health problems, alcohol use is responsible for more than 16,000 traffic fatalities annually, and it plays an important role in violent crime (Felson, Teasdale, & Burchfield, 2008). As almost anyone with an alcoholic family member can attest, alcohol abuse can also cause many problems for families, including domestic violence and divorce and the stress that results from having to deal with someone’s alcoholism on a daily basis. (The Note 7.13 “Children and Our Future” box discusses the impact of parental alcoholism on children.) Alcohol abuse costs the United States more than $185 billion each year in medical expenses, lost earnings because of alcohol-related illness or premature death, lost earnings by victims of violent crime, and alcohol-caused traffic accidents (Harvard School of Public Health, 2012).
Children and Our Future
Children of Alcoholics
As with so many social problems, one of the saddest consequences of alcohol abuse involves children. About one-fifth of children have lived with an alcoholic parent or other adult. Whether because alcoholism is partly inherited or because children tend to use their parents as role models, children of alcoholics are four times more likely than children of nonalcoholics to become alcoholics themselves by the time they reach adulthood.
Because living with an alcoholic parent is often both chaotic and unpredictable, it is no surprise that children of alcoholics often experience a great deal of stress and other difficulties that may also account for their greater tendency to become alcoholics. Compared to other children, they are more likely to be neglected and/or abused by their parents, and they are also more likely to miss school, have lower grades, and engage in disruptive behavior. In addition, they are at great risk for eating disorders and substance abuse other than alcohol abuse. The stress they experience can also harm their neurological development and immune system and put them at greater risk for different kinds of illness and disease. Children of alcoholics are also at greater risk for several kinds of psychological and emotional problems. These include (1) guilt, because they may blame themselves for their parent’s drinking; (2) anxiety, because they worry about their parent’s health and may see their parents arguing and fighting; (3) embarrassment that leads them not to invite friends over to visit nor to ask another adult for help; (4) lack of trust in other people, because they have learned not to trust their alcoholic parent; and (5) anger, confusion, and depression.
One special problem that children of alcoholics face is that they are “forced into adulthood.” They often find themselves having to care for younger siblings and even for their alcoholic parent. By taking on such a heavy responsibility, they in effect become adults at too tender an age. This responsibility weighs on them and helps account for the psychological and emotional difficulties they often experience.
Mental health professionals strongly advise that children of alcoholics receive counseling and other kinds of support to help them deal with their family experiences. Group support programs for teenaged children may be very helpful. Perhaps the best known such program is Alateen, which also services teenagers who want help dealing with an alcoholic friend. Teenagers at Alateen meetings share their experiences, learn how to deal with the special difficulties that stem from having a relative or friend with an alcohol problem, and provide emotional support for each other. One important message they learn from Alateen is that they are in no way responsible for the alcoholism of their parent, other relative, or friend.
Alateen has helped many young people, as this testimonial from “Lizzy” attests: “Alateen has helped me a lot over the years…From the day I went to my first meeting, the door to my happiness was flung open. With the help of the Alateen Group Sponsors and my fellow teens, my life has become what I always wanted it to be. My goal for success in the program was fulfilled. I have been given a second chance at life and I have Alateen to thank for that.”
Young children and teenagers are resilient, but children of alcoholics have to be especially resilient. Programs like Alateen help give them a second chance.
Sources: Alateen, 2011; American Academy of Child and Adolescent Psychiatry, 2006; James, 2008
College Students
Alcohol abuse is also a problem on college and university campuses across the United States. Based on the SAMHSA survey evidence discussed earlier, full-time college students ages 18–22 drink more often and more heavily than their peers who are not in college (Substance Abuse and Mental Health Services Administration, 2008). Among full-time college students ages 18–20, who are all too young to drink legally, about 40 percent have engaged in binge drinking in the past month, and 17 percent have engaged in heavy drinking as defined earlier. Binge drinking on and off campus is so common that binge drinkers consume 91 percent of all the alcohol that college students drink.
Binge drinking by college students has many serious consequences (Center for Science in the Public Interest, 2008; National Center on Addiction and Substance Abuse, 2007). The following are consequences with approximate figures:
- Binge drinkers are much more likely than other students to miss class, get poor grades, be injured, have unprotected sex, and to drive after drinking.
- Six hundred thousand college students suffer alcohol-related injuries (from motor vehicle crashes and other accidents) each year, and 1,700 die from these injuries.
- Thirty thousand college students need medical attention annually to treat alcohol overdosing.
- Seven hundred thousand students are assaulted annually by a student who has been drinking, and three hundred students die from these assaults.
- Students who attend colleges with high rates of binge drinking are more likely to experience sleep disruption, property damage, and physical and sexual assaults than those who attend colleges with low rates of binge drinking.
Tobacco and Nicotine
Nicotine, the major drug in tobacco, is another legal but very dangerous drug. As we saw earlier, its use kills four times as many people every year as those killed by alcohol use. Tobacco is a slow poison. If it were not already a legal drug used by millions, and a company had just manufactured cigarettes for the first time, the Food and Drug Administration would never approve this product. Fortunately for tobacco companies, nicotine does not distort perception the way that alcohol and many other psychoactive drugs do. Someone smoking or otherwise using tobacco can safely drive a car, operate machinery, and so forth, and someone “under the influence” of tobacco does not become violent.

Tobacco is a slow poison. If it were a new drug, it would not be approved for public consumption.
Raul Lieberwirth – cigarette – CC BY-NC-ND 2.0.
If you have ever watched any number of pre-1970s movies or television shows like “Mad Men” that portray life back then, you know that the United States used to have a tobacco culture the way it now has an alcohol culture. Many, many people smoked cigarettes, and a large number smoked cigars or pipes. This particular drug culture began to abate in the 1970s after much evidence mounted about the deaths and other serious health effects of tobacco use and especially about the dangers of second-hand smoke. Whereas college students a generation ago often sat in smoke-filled classrooms and Americans generally sat in smoke-filled restaurants and other venues, today most Americans can count on being in enclosed public spaces in which smoking is banned.
Even so, we have already seen that more than one-fourth of Americans 12 and older, or some 70 million people, are still current users (past month) of tobacco. Almost one-fifth of American adults (18 and older), or 45.3 million adults, smoke cigarettes daily or occasionally (King, Dube, Kaufmann, Shaw, & Pechacek, 2011). Thanks to the greater knowledge about tobacco’s health effects, public education campaigns about these effects, heavy taxes on cigarettes, and changing attitudes about tobacco, these numbers represent a significant decline from a generation ago.
Tobacco use causes more preventable death and illness in the United States than any other cause of death; if no one used tobacco, the more than 400,000 tobacco-related deaths each year would not occur. As we think about tobacco, this startling statistic needs to be kept in mind: About half of all cigarette smokers will one day die from a premature death caused by a smoking-related illness (King et al., 2011). To repeat what was said just earlier, nicotine is a slow poison.
Tobacco kills in several ways. Smoking causes 80–90 percent of all lung cancers, and it greatly increases the risk of emphysema and other lung disease, coronary heart disease, and stroke. In addition to lung cancer, tobacco use also causes several other cancers, including bladder cancer, cervical cancer, esophageal cancer, stomach cancer, and throat cancer. Women who smoke are at greater risk for lower bone density and hip fracture when they get older.
The economics of tobacco use are also worth knowing. Americans spend about $90 billion annually on tobacco products, with most of this amount spent on cigarettes (Centers for Disease Control and Prevention, 2011). They purchase more than 300 billion cigarettes annually, with most of the cigarettes sold by three companies. Cigarette smoking is estimated to cost almost $200 billion annually in medical expenses and lost economic productivity. This works out to a national economic loss of about $10.50 for every pack of cigarettes that is sold.
One interesting and very important fact about the economics of cigarette smoking is what happens when the cost of cigarettes is increased. Most smokers begin their deadly habit during adolescence or young adulthood. Because this is a period of their lives when they do not have much money, increases in the cost of cigarettes are particularly useful in persuading some of these young people not to buy cigarettes. Government data indicate that every 10 percent increase in the price of cigarettes reduces cigarette consumption among young people by 4 percent (Centers for Disease Control and Prevention, 2011). A similar but smaller effect occurs among older smokers.
Earlier we said that the alcohol industry plays a major role in the amount of drinking that occurs in the United States. The same is true of the tobacco industry and smoking. This industry spends about $15 billion annually—or an average of $41 million daily—in advertising, sponsorship of public events, and other activities to promote its deadly product, and for many years hid or distorted data about the deadly effects of cigarette smoking (Brandt, 2009). Because of funding cutbacks during the recent faltering economy, the states have reduced their media campaigns and other efforts aimed at reducing smoking. This reduction, combined with the tobacco industry’s huge promotional spending, leads one public health professor to lament, “The tobacco companies are winning the battle” (Martin, 2011).
Illegal Drugs
The SAMHSA survey also gathers data from its thousands of respondents about illegal drug use. Table 7.4 “Prevalence of Illegal Drug Use, Ages 12 and Older, 2010*” presents these data for several illegal drugs and shows that use of these drugs is far from rare.
Table 7.4 Prevalence of Illegal Drug Use, Ages 12 and Older, 2010*
| Lifetime | Past year | Past month | |
|---|---|---|---|
| Any illegal drug | 47.1 | 15.3 | 8.9 |
| Illegal drug other than marijuana | 30.0 | 8.1 | 3.6 |
| Marijuana/hashish | 41.9 | 11.5 | 6.9 |
| Cocaine/crack | 14.7 | 1.8 | 0.6 |
| Hallucinogens | 14.8 | 1.8 | 0.5 |
| Heroin | 1.6 | 0.2 | 0.1 |
| Stimulants | 8.5 | 1.1 | 0.4 |
| Nonmedical use of prescription-type drugs† | 20.4 | 6.3 | 2.7 |
| * Percentage using in designated time period | |||
| † Includes stimulants | |||
Source: Substance Abuse and Mental Health Services Administration. (2011). Results from the 2010 national survey on drug use and health: Summary of national findings. Rockville, MD: Author.
The following figure from Table 7.5 “Prevalence of Illegal Drug Use, Ages 18–20, 2010*” is striking: 47.1 percent of all Americans ages 12 and older have used an illegal drug at least once in their lifetimes. This percentage translates to almost 120 million people. In terms of lifetime use, the single most popular illegal drug is easily marijuana, but 30 percent of Americans, or 76 million people, have used an illegal drug other than marijuana. Almost 15 percent, or more than 37 million people, have used cocaine/crack or hallucinogens, and more than 20 percent, or almost 52 million people, have used prescription drugs illegally. These percentages and the numbers of people associated with them all indicate that lifetime illegal drug use in the United States is widespread.
Despite this fact, most public health experts are primarily concerned with current (past month) illegal drug use. The percentages for past-month (and also past-year) use in Table 7.5 “Prevalence of Illegal Drug Use, Ages 18–20, 2010*” are noticeably smaller than those for lifetime use. They indicate that most people who have used illegal drugs in their lifetimes are no longer using them, or at least have not used them in the past year or past month. Most of these lifetime users tried their illegal drug once, twice, or a few times and then stopped using it, and some may have used it more often but then stopped. In any event, it is the current, past-month users who raise the most concern for our society in general and for the public health and legal communities and other sectors of our society that deal with illegal drug use and its effects.
In looking at current illegal drug use, we see that 8.9 percent of the public falls into this category. This percentage translates to almost 23 million Americans, no small number by any means. Their favorite illegal drug is marijuana (and hashish), but 3.6 percent, or 9 million people, have used an illegal drug other than marijuana in the past month. These users favor prescription drugs used for nonmedical reasons. Despite the publicity that cocaine/crack still receives, less than 1 percent of the public has used it in the past month, and less than 2 percent has used it in the past year. These small percentages, though, still translate to 1.5 million people and 5.5 million people, respectively.
The percentages in Table 7.4 “Prevalence of Illegal Drug Use, Ages 12 and Older, 2010*” underestimate the problem of illegal drug use in at least two respects. First, the SAMHSA survey does not include people whose illegal drug use is especially high: the homeless, runaway teenagers, jail and prison inmates, and youths in detention centers. Second, and conversely, the SAMHSA survey includes people whose illegal drug use is relatively low—namely, young adolescents and people in their middle age and older years. For this reason, it is instructive to examine the prevalence of illegal drug use among the people who are in their “prime” ages for it: those who are 18–20 years old. Accordingly, Table 7.5 “Prevalence of Illegal Drug Use, Ages 18–20, 2010*” presents the appropriate figures for Americans in this age group.
Table 7.5 Prevalence of Illegal Drug Use, Ages 18–20, 2010*
| Lifetime | Past year | Past month | |
|---|---|---|---|
| Any illegal drug | 52.8 | 37.7 | 23.1 |
| Illegal drug other than marijuana | 31.2 | 19.1 | 8.0 |
| Marijuana/hashish | 46.4 | 32.7 | 20.3 |
| Cocaine/crack | 8.5 | 4.1 | 1.2 |
| Hallucinogens | 14.1 | 7.9 | 2.3 |
| Heroin | 1.6 | 0.5 | 0.2 |
| Stimulants | 7.8 | 3.9 | 1.3 |
| Nonmedical use of prescription-type drugs† | 24.5 | 14.5 | 5.9 |
| * Percentage using in designated time period | |||
| † Includes stimulants | |||
Source: Substance Abuse and Mental Health Services Administration. (2011). Results from the 2010 national survey on drug use and health: Summary of national findings. Rockville, MD: Author.
Take a moment to compare the percentages in Table 7.5 “Prevalence of Illegal Drug Use, Ages 18–20, 2010*” for ages 18–20 to the percentages in Table 7.4 “Prevalence of Illegal Drug Use, Ages 12 and Older, 2010*” for ages 12 and older. When you do this, you will see that past-year and past-month illegal drug use is generally much higher for people ages 18–20 than for everyone 12 and older. More than one-third of the 18–20 age group have used an illegal drug in the past year, and almost one-fourth are current users, having used an illegal drug in the past month. As with the 12 and older population, their drug of choice is clearly marijuana, with nonmedical use of prescription-type drugs a distant second.
This last statement is important to keep in mind. In terms of percentages, the major illegal drug is marijuana. Very low percentages of Americans use other illegal drugs when we consider current use and past-year use, although a greater number have experimented with other illegal drugs in their lifetimes. As we have seen, however, the low percentages for the other illegal drugs still translate into millions of Americans who are current users of illegal drugs other than marijuana. It is also true that drugs like heroin and cocaine/crack are used more heavily in large cities than in smaller cities and towns and rural areas. Although these drugs are only rarely used nationwide, they are a particular problem in large urban areas.
With this backdrop in mind, we now discuss a few illegal drugs in further detail.
Marijuana
As we have seen, marijuana is easily the most widely used illegal drug in the United States. The percentages for marijuana use in Table 7.4 “Prevalence of Illegal Drug Use, Ages 12 and Older, 2010*” translate to 106 million people who have ever used marijuana, 29 million people who used it in the past year, and 17 million people who used it in the past month (current users). As Table 7.5 “Prevalence of Illegal Drug Use, Ages 18–20, 2010*” showed, marijuana use is especially high among young people: One-third of people ages 18–20 have used marijuana in the past year, and one-fifth are current users.
Marijuana use can cause several problems (National Institute on Drug Abuse, 2010). Marijuana distorts perception, impairs coordination, and can cause short-term memory loss, and people who are high from marijuana may be unable to safely drive a motor vehicle or operate machinery. In addition, regular pot smokers are at risk for respiratory problems, though not lung cancer. Chronic marijuana use is also associated with absence from school and the workplace and with social relationship problems, although it is difficult to determine whether marijuana is causing these effects or whether the association exists because someone with personal problems begins using marijuana regularly.
Despite these problems, marijuana is almost certainly the most benign illegal drug in terms of health and social consequences, and it is also much more benign than either alcohol or tobacco (Drug Policy Alliance, 2011; Faupel et al., 2010). As noted earlier, these latter two drugs kill about 520,000 Americans annually. In contrast, marijuana has probably never killed anyone, and its use has not been associated with any cancers. Alcohol use is a risk factor for violent behavior, but marijuana use is a risk factor for mellow behavior; if everyone who now uses alcohol instead smoked marijuana, our violent crime rate would probably drop significantly! Despite some popular beliefs, marijuana is generally not physiologically addictive, it does not reduce ambition and motivation, and it does not act as a “gateway drug” that leads to the use of more dangerous drugs (Hanson, Venturelli, & Fleckenstein, 2012). A review of the evidence on marijuana summarized research findings as follows: “Studies of long-term marijuana smokers do not produce gross or major clinical, psychiatric, psychological, or social difference between users and nonusers, or between heavier and lighter users” (Goode, 2008, p. 247).
While not entirely safe, then, marijuana is much safer, both on an individual basis and on a societal basis, than either alcohol or tobacco. Even so, it remains an illegal drug. This fact underscores our earlier observation that the legality or illegality of drugs has no logical basis. If the personal and social harm caused by a drug determined whether it is legal or not, then it would be logical for marijuana to be legal and for alcohol or tobacco to be illegal.
For better or worse, though, the millions of marijuana users have broken the law. In most states, marijuana possession is a crime punishable by a jail or prison term that depends on the amount of marijuana involved. Fourteen states (Alaska, California, Colorado, Connecticut, Maine, Massachusetts, Minnesota, Mississippi, Nebraska, Nevada, New York, North Carolina, Ohio, Oregon) have decriminalized simple possession of small amounts of marijuana: They treat possession as a minor offense similar to a traffic violation and punish it with only a small fine. Most of these states decriminalized the drug in the 1970s after a national commission with members appointed by the US Congress and by President Richard Nixon recommended taking this action. There is no evidence that marijuana use in these states increased compared to use in the states that have not decriminalized marijuana (Beckett & Herbert, 2008). In fact, marijuana use in the nation declined sharply in the 1980s, the first decade after decriminalization began, both in the states that decriminalized pot possession and in the states that did not decriminalize it.
Cocaine
Cocaine produces a high that is considered more pleasurable than that for any other drug. According to sociologist Erich Goode (2008, p. 288), “Cocaine’s principal effects are exhilaration, elation, and euphoria—voluptuous, joyous feelings accompanied by a sense of grandiosity.” As a stimulant, cocaine also increases energy, alertness, and a sense of self-confidence. It is not physiologically addictive, but it is considered psychologically addictive: The high it produces is so pleasurable that some users find they need to keep using it.
Cocaine is a particularly addictive drug because of the high degree of pleasurable feelings it causes.
Nightlife of Revelry – Cocaine – CC BY 2.0.
Cocaine is made from coca plants grown in South America. It most often appears in a powdered form that is sniffed (or, to use the more common term for this method, snorted). The high it produces takes some time to occur but may last up to thirty minutes once it does arrive. A more potent form, crack cocaine (or, more commonly, crack), is made by heating a mixture of powdered cocaine, baking soda, and water. A user then heats the mixture that remains and breathes in the vapors that result. Crack produces an immediate, intense high and is a relatively inexpensive drug. These features made crack a very popular drug when it was first introduced into US cities in the 1980s (Faupel et al. 2010). Street gangs fought each other to control its distribution and sale, much as organized crime gangs fought each other over alcohol distribution and sale during Prohibition.
Cocaine and crack use has declined since the 1970s and 1980s, but, as Table 7.5 “Prevalence of Illegal Drug Use, Ages 18–20, 2010*” showed, almost 15 percent of the public has used cocaine at least once; this number translates to some 37 million Americans. Still, past-year use is only 1.8 percent, and past-month (current) use is only 0.6 percent. Cocaine use thus must be considered rare in percentage terms. At the same time, these percentages translate to 4.5 million and 1.5 million Americans, respectively. These are not small numbers. Moreover, past-year and past-month cocaine use is higher among young people, as Table 7.5 “Prevalence of Illegal Drug Use, Ages 18–20, 2010*” showed. Further, crack use remains a problem in the nation’s urban areas.
In terms of health risks, cocaine is a much more dangerous drug than marijuana. As a stimulant, cocaine speeds up the central nervous system. Because it does so much more intensely than most other stimulants, its use poses special dangers for the cardiovascular system (National Institute on Drug Abuse, 2011). In particular, it can disrupt the heart’s normal rhythm and cause ventricular fibrillations, and it can speed up the heart and raise blood pressure. An overdose of cocaine can thus be deadly, and long-term use produces an increased risk of stroke, seizure, and heart disease. Because cocaine also constricts blood vessels in the brain, long-term use raises the risk of attention deficit, memory loss, and other cognitive problems. Long-term abuse has also caused panic attacks, paranoia, and even psychosis.
Heroin
Heroin is derived from opium (and more immediately from morphine, an opium derivative) and is almost certainly the most notorious opiate. It was one of the popular opiate drugs that, as discussed earlier, were used so widely during the late nineteenth century. Heroin was first marketed as a painkiller and cough suppressant by the company that makes Bayer aspirin. As the United States became more concerned about opium use, Bayer Laboratories discontinued heroin marketing in 1910, and heroin, like other opiates, was banned under the 1914 Harrison Narcotic Act.
Although Table 7.4 “Prevalence of Illegal Drug Use, Ages 12 and Older, 2010*” shows that its use is minuscule in percentage terms, these percentages translate to 600,000 people who have used heroin in the past year, and 240,000 who have used in the past month. Because these users are concentrated in the nation’s large cities, heroin, like crack, is a special problem for these areas.
Like other narcotics, heroin use produces a feeling of euphoria. After it is injected, “the user feels a flash, a rush, which has been described as an intense, voluptuous, orgasmlike sensation. Following this is the feeling of well-being, tranquility, ease, and calm, the sensation that everything in the user’s life is just fine. Tensions, worries, problems, the rough edges of life—all seem simply to melt away” (Goode, 2008, pp. 308–309).
Although heroin use is uncommon, it continues to capture the public’s concern more than perhaps any other illegal drug. As sociologist Goode (2008, pp. 307–308) has observed,
For decades, it was the most feared, the most dreaded, the “hardest” drug; heroin has virtually defined the drug problem. In spite of being somewhat overshadowed since the mid-1980s by cocaine, and specifically crack, heroin probably remains the single substance the American public is most likely to point to as an example of a dangerous drug. Until recently, disapproval of any level of heroin use was greater than for any other drug. And, until recently, heroin addicts were the most stigmatized of all drug users. Heroin is the epitome of the illicit street drug. Its association in the public mind with street crime, even today, is probably stronger than for any other drug. The stereotype of the junkie is that he or she is by nature a lowlife, an outcast, a “deviant,” a dweller in the underworld, an unsavory, untrustworthy character to be avoided at any cost.
Users typically take heroin into their body by injecting it into a vein. This mode of administration is undoubtedly a major reason for the public’s very negative image of heroin users. Indeed, the image of a heroin addict “shooting up” is one that has appeared in many movies and television shows past and present. Many heroin addicts share their needles, a practice that increases their risk of contracting HIV and hepatitis.
The public’s image and concern about heroin is partly deserved in some ways and partly undeserved in other ways. Like other opiates, heroin is extremely physiologically addictive, although not as addictive as nicotine. But also like other opiates, heroin does not damage body organs. The emaciated look we often associate with heroin users stems not from the drug itself but from the low-caliber lifestyles that heroin addicts tend to live and their decisions to spend the little money they have on heroin rather than on food and a healthier lifestyle. An overdose of heroin can certainly kill, just as overdoses of other drugs can kill. One reason heroin overdoses occur is that heroin users cannot know for sure the purity of the heroin they buy illegally and thus may inject an unsafe dose to get high.
Prescription Drug Abuse
Table 7.4 “Prevalence of Illegal Drug Use, Ages 12 and Older, 2010*” showed that about one-fifth of Americans have used prescription drugs for nonmedical purposes. This type of use is illegal. It constitutes the most widespread illegal drug use other than marijuana use and has grown in recent years, especially among adolescents. The prescription drugs that are most often abused are those containing narcotics, tranquilizers, and stimulants; two of the most common brands that are abused are OxyContin and Vicodin. Because prescription drugs are beneficial for so many people even if they are abused, our nation faces a special difficulty in dealing with the abuse of these drugs. As the head of the National Institute on Drug Abuse explains, “The challenges we face are much more complex because we need to address the needs of patients in pain, while protecting those at risk for substance use disorders” (Zuger, 2011, p. D1). Thus according to a news report, “These drugs must be somehow legal and illegal, encouraged yet discouraged, tightly regulated yet easily available” (Zuger, 2011, p. D1).

Many prescription drug abusers use drugs obtained from their own prescriptions or from prescriptions of friends or relatives.
sharyn morrow – the husband’s vicodin – CC BY-NC-ND 2.0.
Most prescription drug abusers have their own prescriptions or obtain their drugs from friends, acquaintances, or relatives who have their own prescriptions. Whatever the source, some of these prescriptions are obtained legitimately—for actual medical conditions—and then abused, and some are obtained after feigning a medical condition. Many experts fault physicians for overprescribing painkillers and other prescription drugs.
Prescription drug abuse is thought to be growing for two reasons (National Institute on Drug Abuse, 2005). First, physicians’ prescriptions for painkillers and other drugs continue to rise, creating a greater supply of prescription drugs that can be abused. Second, online pharmacies and pain clinics have made it easier to obtain prescription drugs, with or without an actual prescription.
The Note 7.14 “Applying Social Research” box discusses the roots of adolescent prescription drug abuse in family and school factors. The importance of these factors reinforces the sociological view that the origins of drug use often lie beyond the individual and in the social environment.
Applying Social Research
Prescription Drug Abuse by Adolescents
Despite the importance of prescription drug abuse, social science research on its causes is relatively sparse. In one of the first studies to examine the social origins of adolescent prescription drug abuse, sociologist Jason A. Ford analyzed data on adolescents in the national survey conducted by the Substance Abuse and Mental Health Services Administration that is discussed elsewhere in this chapter. Drawing on the large body of work that attributes drug use in part to weak social bonds, Ford reasoned that prescription drug abuse should be higher among adolescents who have weaker bonds to their parents and also weaker bonds to their schools.
For his measure of parental bonds, Ford used several questions that asked adolescents about their relationship with their parents, including whether parents feel proud of them and praise them for doing a good job, and whether their parents help them with their homework and limit their time out with friends on a school night. For his measure of school bonds, he used several questions that asked adolescents such things as whether they liked going to school and whether they found their schooling meaningful and important. His measure of prescription drug abuse relied on the adolescents’ self-reports of whether they had used any prescription drug for nonmedical purposes in the past year.
Controlling for gender, race, and other factors, Ford found support for his hypotheses: prescription drug abuse was higher among adolescents with weaker bonds to their parents and also weaker bonds to their schools.
These results have important implications for efforts to reduce prescription drug abuse by adolescents. They suggest that efforts by our society to strengthen families and to improve our schools may well have a significant, beneficial side-effect: lower prescription drug abuse by adolescents.
Source: Ford, 2009
Key Takeaways
- The distinction between legal drugs and illegal drugs has no logical basis; legal drugs cause much more harm than illegal drugs.
- Alcohol and tobacco kill more than 500,000 Americans annually. Binge drinking on campuses results in accidents and assaults involving several hundred thousand college students annually.
- Marijuana is by far the most commonly used illegal drug. The low prevalence of other illegal drugs still amounts to millions of people using these drugs annually.
For Your Review
- Do you agree or disagree that the distinction between legal drugs and illegal drugs is not logical? Explain your answer.
- Do you agree that binge drinking is a problem that campuses should address, or do you think that it’s a relatively harmless activity that lets students have some fun? Explain your answer.
References
Alateen. (2011). Am I a peacemaker or a creator of chaos. Alateen Talk. Retrieved from http[0]://www.al-anon.org/alateen-talk.
American Academy of Child and Adolescent Psychiatry. (2006). Children of alcoholics. Retrieved October 4, 2011, from http://www.aacap.org/galleries/FactsForFamilies/17_children_of_alchoholics.pdf.
American Medical Association. (2004). Alcohol industry 101: Its structure & organization. Chicago, IL: Author.
Beckett, K., & Herbert, S. (2008). The consequences and costs of marijuana prohibition. Seattle, WA: American Civil Liberties Union of Washington State.
Brandt, A. (2009). The cigarette century: The rise, fall, and deadly persistence of the product that defined America. New York, NY: Basic Books.
Center for Science in the Public Interest. (2008). Binge drinking on college campuses. Retrieved September 20, 2011, from http://www.cspinet.org/booze/collfact1.htm.
Centers for Disease Control and Prevention. (2011). Economic facts about US tobacco production and use. Retrieved September 20, 2011, from http://www.cdc.gov/tobacco/data_statistics/fact_sheets/economics/econ_facts/.
Distilled Spirits Council of the United States. (2011). Economic contribution of alcohol beverage industry. Retrieved September 19, 2011, from http://www.discus.org/pdf/ATT2_Economic_Contribution.pdf.
Drug Policy Alliance. (2011). Marijuana facts. Retrieved September 22, 2011, from http://www.drugpolicy.org/facts/drug-facts/marijuana-facts.
Faupel, C. E., Horowitz, A. M., & Weaver., G. S. (2010). The sociology of American drug use. New York, NY: Oxford University Press.
Felson, R. B., Teasdale, B., & Burchfield, K. B. (2008). The influence of being under the influence. Journal of Research in Crime & Delinquency, 45(2), 119–141.
Ford, J. A. (2009). Nonmedical Prescription Drug Use Among Adolescents: The Influence of Bonds to Family and School. Youth & Society, 40(3), 336–352.
Frech, E. J., & Go, M. F. (2009). Treatment and Chemoprevention of NSAID-associated Gastrointestinal Complications. Therapeutics and Clinical Risk Management, 5, 65–73.
Gardner, A. (2010, May 3). Report: Alcohol Companies go online to lure young drinkers. USA Today. Retrieved from http://www.usatoday.com/news/health/index.
Goode, E. (2008). Drugs in American society (7th ed.). New York, NY: McGraw Hill.
Hanson, G. R., Venturelli, P. J., & Fleckenstein, A. E. (2012). Drugs and society (11th ed.). Burlington, MA: Jones & Bartlett.
Harvard School of Public Health. (2012). Alcohol: Balancing risks and benefits. Retrieved March 30, 2012, from http://www.hsph.harvard.edu/nutritionsource/what-should-you-eat/alcohol-full-story/index.html.
James, S. D. (2008, September 10). Children of alcoholics forced into adulthood. abcnews.com. Retrieved from http://abcnews.go.com/Health/story?id=5770753&page=5770751.
Jernigan, D. H. (2009). The global alcohol industry: An overview [Supplmental material]. Addiction, 104, 6–12.
King, B., Dube, S., Kaufmann, R., Shaw, L., & Pechacek, T. (2011). Vital signs: Current cigarette smoking among adults aged ≥18 years—United States, 2005–2010. Morbidity and Mortality Weekly Report, 60(35), 1207–1212.
Kleiman, M. A. R., Caulkins, J. P., & Hawken, A. (2011). Drugs and drug policy: What everyone needs to know. New York, NY: Oxford University Press.
Martin, T. W. (2011, September 6). Fewer Americans are smoking, and those who do puff less. The Wall Street Journal. Retrieved from http://blogs.wsj.com/health/2011/2009/2006/fewer-americans-are-smoking-and-those-who-do-puff-less/.
Mokdad, A. H., Marks, J. S., Stroup, D. F., & Gerberding, J. L. (2004). Actual causes of death in the United States, 2000. Journal of the American Medical Association, 291(10), 1238–1245.
National Center on Addiction and Substance Abuse. (2007). Wasting the best and the brightest: Substance abuse at America’s colleges and universities. New York, NY: Author.
National Institute on Drug Abuse. (2005). Prescription drugs: Abuse and addiction. Washington, DC: Author.
National Institute on Drug Abuse. (2010). InfoFacts: Marijuana. Retrieved September 22, 2011, from http://www.nida.nih.gov/infofacts/marijuana.html.
National Institute on Drug Abuse. (2011). Cocaine: Abuse and addiction. Retrieved September 27, 2011, from http://www.nida.nih.gov/researchreports/cocaine/effects.html.
National Institutes of Health. (2011). NIH study finds hospitalizations increase for alcohol and drug overdoses. Retrieved September 21, 2011, from http://www.nih.gov/news/health/sep2011/niaaa-20.htm.
Smith, A. (2011, June 9). Alcohol Sales Thrive in Hard Times. CNN. Retrieved from http://money.cnn.com.
Substance Abuse and Mental Health Services Administration. (2008). Underage alcohol use among full-time college students. Retrieved September 20, 2011, from http://oas.samhsa.gov/2k6/college/collegeUnderage.htm.
US Department of Agriculture. (2011). Food CPI and expenditures: Table 1. Retrieved September 19, 2011, from http://www.ers.usda.gov/Briefing/CPIFoodAndExpenditures/Data/Expenditures_tables/table1.htm.
Zuger, A. (2011, June 14). A general in the drug war. New York Times. p. D1.
