13.3 Problems of Health in the United States
Learning Objectives
- Describe how and why social class, race and ethnicity, and gender affect physical health and health care in the United States.
- Summarize the differences that social class, race and ethnicity, and gender make for mental health.
When we examine health and health care in the United States, there is both good news and bad news. The good news is considerable. Health has improved steadily over the last century, thanks in large part to better public sanitation and the discovery of antibiotics. Illnesses and diseases such as pneumonia and polio that used to kill or debilitate people are either unknown today or treatable by modern drugs. Other medical discoveries and advances have also reduced the extent and seriousness of major illnesses, including many types of cancer, and have prolonged our lives.

Cigarette smoking in the United States has declined considerably since the 1960s.
Xava du – smoke souls – CC BY-NC-ND 2.0.
Because of these and other factors, the US average life expectancy climbed from about 47 years in 1900 to about 78 years in 2010. Similarly, infant mortality dropped dramatically in the last half-century from 29.2 infant deaths per 1,000 live births in 1950 to only 6.75 in 2007 (see Figure 13.4 “Infant Deaths per 1,000 Live Births, United States, 1950–2007”). Cigarette smoking declined from 51 percent for males and 34 percent for females in 1965 to 23 percent and 18 percent, respectively, in 2009 (National Center for Health Statistics, 2011). In another area, various policies during the past three decades have dramatically reduced levels of lead in young children’s blood: 88 percent of children had unsafe levels in the mid-1970s, compared to less than 2 percent three decades later (Centers for Disease Control and Prevention, 2007).
Figure 13.4 Infant Deaths per 1,000 Live Births, United States, 1950–2007
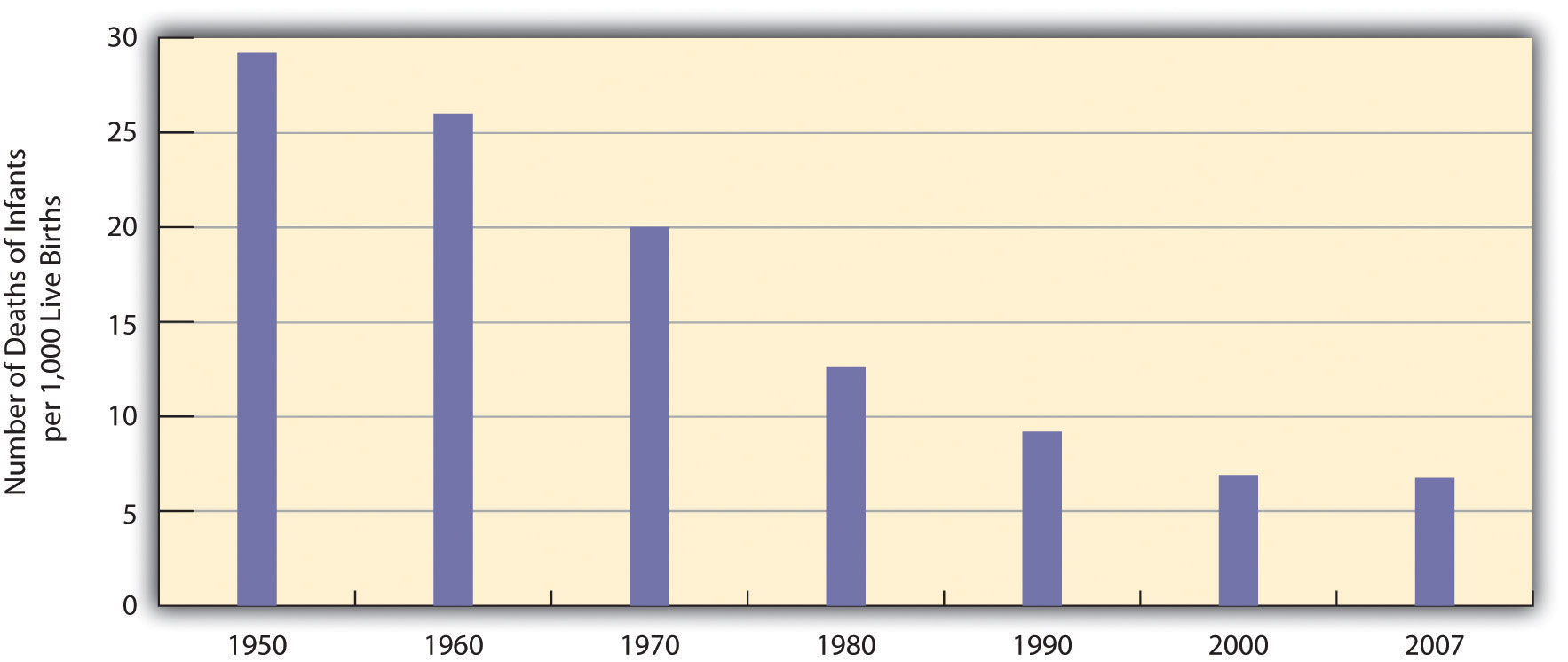
Source: Data from National Center for Health Statistics. (2011). Health, United States, 2010. Hyattsville, MD: Centers for Disease Control and Prevention.
The Poor Status of American Health
Unfortunately, the bad news is also considerable. Despite all the gains just mentioned, the United States lags behind most other wealthy democracies in several health indicators, as we have seen, even though it is the wealthiest nation in the world. Moreover, 14.5 percent of US households and almost 49 million Americans are “food insecure” (lacking sufficient money for adequate food and nutrition) at least part of the year; more than one-fifth of all children live in such households (Coleman-Jensen, Nord, Andrews, & Carlson, 2011). More than 8 percent of all infants are born at low birth weight (under 5.5 pounds), putting them at risk for long-term health problems; this figure has risen steadily since the late 1980s and is higher than the 1970 rate (National Center for Health Statistics, 2011). In other areas, childhood rates of obesity, asthma, and some other chronic conditions are on the rise, with about one-third of children considered obese or overweight (Van Cleave, Gortmaker, & Perrin, 2010). Clearly the United States still has a long way to go in improving the nation’s health.
There is also bad news in the social distribution of health. Health problems in the United States are more often found among the poor, among people from certain racial and ethnic backgrounds, and, depending on the problem, among women or men. Social epidemiology refers to the study of how health and illness vary by sociodemographic characteristics, with such variations called health disparities. When we examine social epidemiology in the United States, we see that many health disparities exist. In this way, health and illness both reflect and reinforce society’s social inequalities. We now turn to the most important health disparities, starting with physical health and then mental health.
Health Disparities: Physical Health
Social Class
Not only do the poor have less money, but they also have much worse health, as the news story that began this chapter illustrated. There is growing recognition in the government and in medical and academic communities that social class makes a huge difference when it comes to health and illness (Centers for Disease Control and Prevention, 2011).
Many types of health indicators illustrate the social class–health link in the United States. In an annual survey conducted by the government, people are asked to indicate the quality of their health. As Figure 13.5 “Family Income and Self-Reported Health (Percentage of People 18 or Over Saying Health Is Only Fair or Poor), 2009” shows, poor people are much more likely than those with higher incomes to say their health is only fair or poor. These self-reports of health are subjective indicators, and it is possible that not everyone interprets “fair” or “poor” health in the same way. But objective indicators of actual health also indicate a strong social class–health link (National Center for Health Statistics, 2011).
Figure 13.5 Family Income and Self-Reported Health (Percentage of People 18 or Over Saying Health Is Only Fair or Poor), 2009
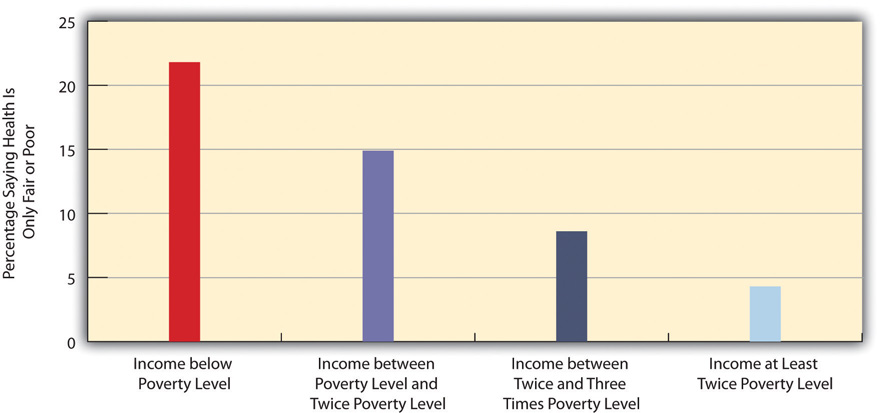
Source: Data from National Center for Health Statistics. (2011). Health, United States, 2010. Hyattsville, MD: Centers for Disease Control and Prevention.
Children and Our Future
The Poor Health of Poor Children
When we consider health disparities, some of the most unsettling evidence involves children. As a recent report by the Robert Wood Johnson Foundation concluded, “The data illustrate a consistent and striking pattern of incremental improvements in health with increasing levels of family income and educational attainment: As family income and levels of education rise, health improves. In almost every state, shortfalls in health are greatest among children in the poorest or least educated households, but even middle-class children are less healthy than children with greater advantages.”
Some government data illustrate the difference that poverty makes for the nation’s children:
- Children of poor mothers are more than twice as likely as children born to wealthier mothers to be born with low birth weight.
- By the age of 9 months, poor children are already more likely to exhibit poor health and lower cognitive and socioemotional development.
- By age 3, poor children are two-thirds more likely to have asthma than children whose families’ incomes are more than 150 percent of the poverty line.
- Based on their parents’ reports, poor children are almost five times more likely (33 percent compared to 7 percent) to be in less than very good health (i.e., their parents rated their children’s health as poor, fair, or good rather than as very good or excellent).
In these and other ways, children in low-income families are more likely than children in wealthier families to have more health problems, many of which last into adolescence and adulthood. Poor children’s poor health thus makes a critical difference throughout their lives. As sociologist Steven A. Haas and colleagues observe, “A growing body of work demonstrates that those who experience poor health early in life go on to complete less schooling, hold less prestigious jobs, and earn less than their healthier childhood peers.”
One reason for the poor health of poor children is that their families are more likely to experience many kinds of stress (see Chapter 2 “Poverty”). Another reason is that their families are more likely to experience food insecurity and, if they are urban, to live in neighborhoods with higher levels of lead and pollution. Low-income children also tend to watch television more often than wealthier children and for this and other reasons to be less physically active; their relative lack of physical activity is yet another reason for their worse health. Finally, their parents are much more likely than wealthier parents to smoke cigarettes; the secondhand smoke they inhale impairs their health.
The clear evidence of poverty’s effects on the health of poor children underscores the need of the United States to do everything possible to minimize these effects. Any money spent to reduce these effects will pay for itself many times over throughout these children’s lifetimes: They will have fewer health problems as they grow up, costing the United States much less in health care, and be better able to do well in school and to have higher incomes as adults. In both the short run and long run, then, improving the health of poor children will also improve the economic and social health of the whole nation.
Sources: Haas, Glymour, & Berkman, 2011; Kaplan, 2009; Murphey, Mackintosh, & McCoy-Roth, 2011; Robert Wood Johnson Foundation, 2008
For example, poor adults are also at much greater risk for many health problems, including heart disease, diabetes, arthritis, and some types of cancer. Rates of high blood pressure, serious heart conditions, and diabetes are at least twice as high for middle-aged adults with family incomes below the poverty level than for those with incomes at least twice the poverty level. All these social class differences in health contribute to a striking difference in life expectancy, with Americans whose family incomes are more than four times the federal poverty level expected to live 6.5 years longer than those living in poverty (Kaplan, 2009).
Several reasons account for the social class–health link (Pampel, Krueger, & Denney, 2010). One reason is stress, which, as Chapter 2 “Poverty” explained, is higher for people with low incomes because of unemployment, problems in paying for the necessities of life, and a sense of little control over what happens to them. Stress in turn damages health because it impairs the immune system and other bodily processes.
A second reason is that poor people live in conditions, including crowded, dilapidated housing with poor sanitation, that are bad for their health and especially that of their children. Although these conditions have improved markedly in the United States over the last few decades, they continue for many of the poor.
Another reason for the poor’s worse health is their lack of access to adequate health care. As is well known, many poor people lack medical insurance and in other respects have inadequate health care. These problems make it more likely they will become ill in the first place and more difficult for them to become well because they cannot afford to visit a physician or to receive other health care. Still, social class disparities in health exist even in countries that provide free national health care, a fact that underscores the importance of the other reasons discussed here for the social class–health link (Elo, 2009).

Many people who are poor or near poor lack medical insurance and in other ways have inadequate health care. These problems make it more likely they will become ill and, once ill, less likely they will become well.
Truthout.org – Money Behind Health Care – CC BY-NC-SA 2.0.
A fourth reason is a lack of education, which, in ways not yet well understood, leads poor people to be unaware or unconcerned about risk factors for health and to have a fatalistic attitude that promotes unhealthy behaviors and reluctance to heed medical advice (Elo, 2009). In one study of whether smokers quit smoking after a heart attack, only 10 percent of heart attack patients without a high school degree quit smoking, compared to almost 90 percent of those with a college degree (Wray, Herzog, Willis, & Wallace, 1998).
A final reason for the poor health of poor people is unhealthy lifestyles, as just implied. Although it might sound like a stereotype, poor people are more likely to smoke, to eat high-fat food, to avoid exercise, to be overweight, and, more generally, not to do what they need to do (or to do what they should not be doing) to be healthy (Pampel et al., 2010). Scholars continue to debate whether unhealthy lifestyles are more important in explaining poor people’s poor health than the other factors just discussed. Regardless of the proper mix of reasons, the fact remains that the poor have worse health.
Race and Ethnicity
Health differences also exist when we examine the effects of race and ethnicity, and they are literally a matter of life and death. We can see this when we compare life expectancies for whites and African Americans born in 2006 (Table 13.2 “US Life Expectancy at Birth for People Born in 2007”). When we do not take gender into account, African Americans can expect to live about five fewer years than whites. Among men, they can expect to live almost six fewer years, and among women, four fewer years.
Table 13.2 US Life Expectancy at Birth for People Born in 2007
| African American | Both sexes | 73.6 |
| Men | 70.0 | |
| Women | 76.8 | |
| White | Both sexes | 78.4 |
| Men | 75.9 | |
| Women | 80.8 |
Source: Data from National Center for Health Statistics. (2011). Health, United States, 2010. Hyattsville, MD: Centers for Disease Control and Prevention.
At the beginning of the life course, infant mortality also varies by race and ethnicity (Table 13.3 “Mother’s Race/Ethnicity and US Infant Mortality, 2006 (Number of Infant Deaths per 1,000 Live Births)”), with African American infants more than twice as likely as white infants to die before their first birthday. Infant mortality among Native Americans is almost 1.5 times the white rate, while that for Latinos is about the same (although the Puerto Rican rate is also higher, at 8.0), and Asians a bit lower. In a related indicator, maternal mortality (from complications of pregnancy or childbirth) stands at 8.1 maternal deaths for every 100,000 live births for non-Latina white women, 7.2 for Latina women, and a troubling 23.8 for African American women. Maternal mortality for African American women is thus about three times greater than that for the other two groups.
Table 13.3 Mother’s Race/Ethnicity and US Infant Mortality, 2006 (Number of Infant Deaths per 1,000 Live Births)
| African American | 12.9 |
| Asian or Pacific Islander | 4.5 |
| Latina | 5.4 |
| Central and South American | 4.5 |
| Cuban | 5.1 |
| Mexican | 5.3 |
| Puerto Rican | 8.0 |
| Native American | 8.3 |
| White | 5.6 |
Source: Data from National Center for Health Statistics. (2011). Health, United States, 2010. Hyattsville, MD: Centers for Disease Control and Prevention.
In other indicators, African Americans are more likely than whites to die from heart disease, although the white rate of such deaths is higher than the rates of Asians, Latinos, and Native Americans. African Americans are also more likely than whites to be overweight and to suffer from asthma, diabetes, high blood pressure, and several types of cancer. Latinos and Native Americans have higher rates than whites of several illnesses and conditions, including diabetes.
Commenting on all these disparities in health, a former head of the US Department of Health and Human Services said a decade ago, “We have been—and remain—two nations: one majority, one minority—separated by the quality of our health” (Penn et al., 2000, p. 102). The examples just discussed certainly indicate that her statement is still true today.
Why do such large racial and ethnic disparities in health exist? To a large degree, they reflect the high poverty rates for African Americans, Latinos, and Native Americans compared to those for whites. In addition, inadequate medical care is perhaps a special problem for people of color, thanks to unconscious racial bias among health-care professionals that affects the quality of care that people of color receive (see discussion later in this chapter).
An additional reason for racial disparities in health is diet. Many of the foods that have long been part of African American culture are high in fat. Partly as a result, African Americans are much more likely than whites to have heart disease and high blood pressure and to die from these conditions (Parra-Medina et al., 2010). In contrast, first-generation Latinos tend to have diets consisting of beans, grains, and other low-fat foods, preventing health problems stemming from their poverty from being even worse. But as the years go by and they adopt the typical American’s eating habits, their diets tend to worsen, and their health worsens as well (Pérez-Escamilla, 2009).
In a significant finding, African Americans tend to have worse health than whites even among those with the same incomes. Several reasons explain this racial gap. One is the extra stress that African Americans of all incomes face because they live in a society that is still racially prejudiced and discriminatory (Bratter & Gorman, 2011). In this regard, studies find that African Americans and Latinos who have experienced the most racial discrimination in their daily lives tend to have worse physical health (Lee & Ferraro, 2009). Some middle-class African Americans may also have grown up in poor families and incurred health problems in childhood that continue to affect them. As a former US surgeon general once explained, “You’re never dealing with a person just today. You’re dealing with everything they’ve been exposed to throughout their lives. Does it ever end? Our hypothesis is that it never ends” (Meckler, 1998, p. 4A).

African Americans have worse health than whites, even when people with the same incomes are compared. One reason for this racial gap is the continuing racial discrimination that African Americans experience and the stress that accompanies this experience.
Pixabay – CC0 Public Domain.
To some degree, racial differences in health may also have a biological basis. For example, African American men appear to have higher levels of a certain growth protein that may promote prostate cancer; African American smokers may absorb more nicotine than white smokers; and differences in the ways African Americans’ blood vessels react may render them more susceptible to hypertension and heart disease (Meckler, 1998; Ricker & Bird, 2005). Because alleged biological differences have been used as the basis for racism, and because race is best thought of as a social construction rather than a biological concept (see Chapter 3 “Racial and Ethnic Inequality”), we must be very careful in acknowledging such differences (Frank, 2007). However, if they do indeed exist, they may help explain at least some of the racial gap in health.
A final factor contributing to racial differences in health is physical location: poor people of color are more likely to live in urban areas and in other locations that are unhealthy places because of air and water pollution, hazardous waste, and other environmental problems (Walker, 2011). This problem is termed environmental racism (Michney, 2011). One example of this problem is found in the so-called Cancer Alley on a long stretch of the Mississippi River in Louisiana populated mostly by African Americans; 80 percent of these residents live within three miles of a polluting industrial facility (Cernansky, 2011).
Gender
The evidence on gender and health is both complex and fascinating. Women outlive men by more than six years, and, as Table 13.2 “US Life Expectancy at Birth for People Born in 2007” showed, the gender difference in longevity persists across racial categories. At the same time, women have worse health than men in many areas. For example, they are more likely to suffer from migraine headaches, osteoporosis, and immune diseases such as lupus and rheumatoid arthritis. Women thus have more health problems than men do even though they outlive men—a situation commonly known as the morbidity paradox (Gorman & Read, 2006). Why, then, do women outlive men? Conversely, why do men die earlier than women? The obvious answer is that men have more life-threatening diseases, such as heart disease and emphysema, than women, but that raises the question of why this is so.
Several reasons explain the gender gap in longevity. One might be biological, as women’s estrogen and other sex-linked biological differences may make them less susceptible to heart disease and other life-threatening illnesses, even as they render them more vulnerable to some of the health problems already listed (Kuller, 2010). A second reason is that men lead more unhealthy lifestyles than women because of differences in gender socialization. For example, men are more likely than women to smoke, to drink heavily, and to drive recklessly. All such behaviors make men more vulnerable than women to life-threatening illnesses and injuries. Men are also more likely than women to hold jobs in workplaces filled with environmental and safety hazards that kill thousands of people—most of them men—annually.
A final reason is men’s reluctance to discuss and seek help for their medical problems, owing to their masculine socialization into being “strong, silent types.” Just as men do not like to ask for directions, as the common wisdom goes, so do they not like to ask for medical help. As one physician put it, “I’ve often said men don’t come in for checkups because they have a big S tattooed on their chests; they think they’re Superman” (Guttman, 1999, p. 10).
Studies find that men are less likely than women to tell anyone when they have a health problem and to seek help from a health-care professional (Emmers-Sommer et al., 2009). When both sexes do visit a physician, men ask fewer questions than women do. In one study, the average man asked no more than two questions, while the average woman asked at least six. Because patients who ask more questions get more information and recover their health more quickly, men’s silence in the exam room may contribute to their shorter longevity (Foreman, 1999). Interestingly, the development of erectile dysfunction drugs like Viagra may have helped improve men’s health, as men have had to see a physician to obtain prescriptions for these drugs when otherwise they would not have seen a physician (Guttman, 1999).
We have just discussed why men die sooner than women, which is one of the two gender differences that constitute the morbidity paradox. The other gender difference concerns why women have more nonfatal health problems than men. Several reasons explain this difference (Read & Gorman, 2010).

Women more than men tend to have more health problems that are not life threatening. Two reasons for this gender difference are gender inequality in the larger society and the stress accompanying women’s traditional caregiving role in the family.
Francisco Osorio – CL Society 287: Waiting for a doctor – CC BY 2.0.
One reason arises from the fact that women outlive men. Because women are thus more likely than men to be in their senior years, they are also more likely to develop the many health problems associated with old age. This suggests that studies that control for age (by comparing older women with older men, middle-aged women with middle-aged men, and so forth) should report fewer gender differences in health than those that do not control for age, and this is indeed true.
However, women still tend to have worse health than men even when age is taken into account. Medical sociologists attribute this gender difference to the gender inequality in the larger society (Read & Gorman, 2010). For example, women are poorer overall than men, as they are more likely to work only part-time and in low-paying jobs even if they work full time. As discussed earlier in this chapter, poverty is a risk factor for health problems. Women’s worse health, then, is partly due to their greater likelihood of living in poverty or near poverty. Because of their gender, women also are more likely than men to experience stressful events in their everyday lives, such as caring for a child or an aging parent. Their increased stress impairs the immune systems and thus worsens their health. It also is an important cause of their greater likelihood of depression and the various physical health problems (weakened immune systems, higher blood pressure, lack of exercise) that depression often causes. Finally, women experience discrimination in their everyday lives because of our society’s sexism, and (as is also true for people of color) this discrimination is thought to produce stress and thus poorer physical health (Landry & Mercurio, 2009).
Health Disparities: Mental Health
Health consists of mental well-being as well as physical well-being, and people can suffer mental health problems in addition to physical health problems. Scholars disagree over whether mental illness is real or, instead, a social construction. The predominant view in psychiatry, of course, is that people do have actual problems in their mental and emotional functioning and that these problems are best characterized as mental illnesses or mental disorders and should be treated by medical professionals (McNally, 2011). But other scholars say mental illness is a social construction or a “myth” (Szasz, 2010). In their view, all kinds of people sometimes act oddly, but only a few are labeled as mentally ill. If someone says she or he hears the voice of an angel, we ordinarily attribute their perceptions to their religious views and consider them religious, not mentally ill. But if someone instead insists that men from Mars have been in touch, we are more apt to think there is something mentally wrong with that person. Mental illness thus is not real but rather is the reaction of others to problems they perceive in someone’s behavior.
This intellectual debate notwithstanding, many people do suffer serious mental and emotional problems, such as severe mood swings and depression, that interfere with their everyday functioning and social interaction. Sociologists and other researchers have investigated the social epidemiology of these problems. Several generalizations seem warranted from their research regarding disparities in mental health (Cockerham, 2011).
Social Class
First, social class affects the incidence of mental illness. To be more specific, poor people exhibit more mental health problems than richer people: They are more likely to suffer from schizophrenia, serious depression, and other problems. A major reason for this link is the stress of living in poverty and the many living conditions associated with it. One interesting causal question here is whether poverty leads to mental illness or mental illness leads to poverty. Although there is evidence of both causal paths, most scholars believe that poverty contributes to mental illness more than the reverse (Warren, 2009).

Women are more likely than men to be seriously depressed. Sociologists attribute this gender difference partly to gender socialization that leads women to keep problems inside themselves while encouraging men to express their problems outwardly.
Jessica B – Week Five – Face of depression… – CC BY-NC-ND 2.0.
Race and Ethnicity
Second, there is no clear connection between race/ethnicity and mental illness, as evidence on this issue is mixed: Although many studies find higher rates of mental disorder among people of color, some studies find similar rates to whites’ rates (Mossakowski, 2008). These mixed results are somewhat surprising because several racial/ethnic groups are poorer than whites and more likely to experience everyday discrimination, and for these reasons should exhibit more frequent symptoms of mental and emotional problems. Despite the mixed results, a fair conclusion from the most recent research is that African Americans and Latinos are more likely than whites to exhibit signs of mental distress (Jang, Chiriboga, Kim, & Phillips, 2008; Mossakowski, 2008).
Gender
Third, gender is related to mental illness but in complex ways, as the nature of this relationship depends on the type of mental disorder. Women have higher rates of manic-depressive disorders than men and are more likely to be seriously depressed, but men have higher rates of antisocial personality disorders that lead them to be a threat to others (Kort-Butler, 2009). Although some medical researchers trace these differences to sex-linked biological differences, sociologists attribute them to differences in gender socialization that lead women to keep problems inside themselves while encouraging men to express their problems outwardly, as through violence. To the extent that women have higher levels of depression and other mental health problems, the factors that account for their poorer physical health, including their higher rates of poverty and stress and rates of everyday discrimination, are thought to also account for their poorer mental health (Read & Gorman, 2010).
Key Takeaways
- Social class, race and ethnicity, and gender all influence the quality of health in the United States. Health problems are more common among people from low-income backgrounds and among people of color. Women are more likely than men to have health problems that are not life threatening.
- Although debate continues over whether mental illness is a social construction, many people do suffer mental health problems. The social epidemiology for mental health and illness resembles that for physical health and illness, with social class, race/ethnicity, and gender disparities existing.
- The private insurance model in the United States incurs huge administrative costs and results in more than 50 million people lacking health insurance.
For Your Review
- In thinking about the health problems of individuals from low-income backgrounds, some people blame lack of access to adequate health care for these problems, while other people blame unhealthy lifestyles practiced by low-income individuals. Where do you stand on this debate? Explain your answer.
- Write a brief essay in which you present a sociological explanation of the higher rate of depression found among women than among men.
References
Bratter, J. L., & Gorman, B. K. (2011). Is discrimination an equal opportunity risk? Racial experiences, socioeconomic status, and health status among black and white adults. Journal of Health and Social Behavior, 52, 365–382.
Centers for Disease Control and Prevention. (2007). Interpreting and managing blood lead levels <10 μg/dL in children and reducing childhood exposures to lead: Recommendations of CDC’s advisory committee on childhood lead poisoning prevention. MMWR (Morbidity and Mortality Weekly Report), 56(RR-8), 1–16.
Centers for Disease Control and Prevention. (2011). CDC health disparities and inequalities report—United States, 2011. Morbidity and Mortality Weekly Report, 60, 1–114.
Cernansky, R. (2011, February 8). Cancer alley: Big industry & bigger illness along Mississippi River. Retrieved from http://www.treehugger.com/corporate-responsibility/cancer-alley-big-industry-bigger-illness-along-mississippi-river.html.
Cockerham, W. C. (2011). Sociology of mental disorder (8th ed.). Upper Saddle River, NJ: Prentice Hall.
Coleman-Jensen, A., Nord, M., Andrews, M., & Carlson, S. (2011). Household food security in the United States in 2010. Washington, DC: US Department of Agriculture.
Elo, I. T. (2009). Social class differentials in health and mortality: Patterns and explanations in comparative perspective. Annual Review of Sociology, 35, 553–572.
Emmers-Sommer, T. M., Nebel, S., Allison, M.-L., Cannella, M. L., Cartmill, D., Ewing, S., et al. (2009). Patient-provider communication about sexual health: The relationship with gender, age, gender-stereotypical beliefs, and perceptions of communication inappropriateness. Sex Roles: A Journal of Research, 60, 9–10.
Foreman, J. (1999, June 14). A vist most men would rather not make. The Boston Globe, p. C1.
Frank, R. (2007). What to make of it? The (Re)emergence of a biological conceptualization of race in health disparities research. Social Science & Medicine, 64(10), 1977–1983.
Gorman, B. K., & Read, J. G. (2006). Gender disparities in adult health: An examination of three measures of morbidity. Journal of Health and Social Behavior, 47(2), 95–110.
Guttman, M. (1999, June 11–13). Why more men are finally going to the doctor. USA Weekend, p. 10.
Haas, S. A., Glymour, M., & Berkman, L. F. (2011). Childhood health and labor market inequality over the life course. Journal of Health and Social Behavior, 52, 298–313.
Jang, Y., Chiriboga, D. A., Kim, G., & Phillips, K. (2008). Depressive symptoms in four racial and ethnic groups: The survey of older Floridians (SOF). Research on Aging, 30(4), 488–502.
Kaplan, G. A. (2009). The poor pay more: Poverty’s high cost to health. Princeton, NJ: Robert Wood Johnson Foundation.
Kort-Butler, L. A. (2009). Coping styles and sex differences in depressive symptoms and delinquent behavior. Journal of Youth and Adolescence, 38(1), 122–136.
Kuller, L. H. (2010). Cardiovascular disease is preventable among women. Expert Review of Cardiovascular Therapy, 8(2), 175–187.
Landry, L. J., & Mercurio, A. E. (2009). Discrimination and women’s mental health: The mediating role of control. Sex Roles: A Journal of Research, 61, 3–4.
Lee, M.-A., & Ferraro, K. F. (2009). Perceived discrimination and health among Puerto Rican and Mexican Americans: Buffering effect of the lazo matrimonial? Social Science & Medicine, 68, 1966–1974.
McNally, R. J. (2011). What is mental illness? Cambridge, MA: Belknap Press.
Meckler, L. (1998, November 27). Health gap between races persists. Ocala Star-Banner, p. 4A.
Michney, T. M. (2011). White civic visions versus black suburban aspirations: Cleveland’s Garden Valley urban renewal project. Journal of Planning History, 10(4), 282–309.
Mossakowski, K. N. (2008). Dissecting the influence of race, ethnicity, and socioeconomic status on mental health in young adulthood. Research on Aging, 30(6), 649–671.
Murphey, D., Mackintosh, B., & McCoy-Roth, M. (2011). Early childhood policy focus: Health eating and physical activity. Early Childhood Highlights, 2(3), 1–9.
National Center for Health Statistics. (2011). Health, United States, 2010. Hyattsville, MD: Centers for Disease Control and Prevention.
Pampel, F. C., Krueger, P. M., & Denney, J. T. (2010). Socioeconomic disparities in health behaviors. Annual Review of Sociology, 36, 349–370.
Parra-Medina, D., Wilcox, S., Wilson, D. K., Addy, C. L., Felton, G., & Poston, M. B. (2010). Heart healthy and ethnically relevant (HHER) lifestyle trial for improving diet and physical activity in underserved African American women. Contemporary Clinical Trials, 31(1), 92–104.
Penn, N. E., Kramer, J., Skinner, J. F., Velasquez, R. J., Yee, B. W. K., Arellano, L. M., et al. (2000). Health practices and health-care systems among cultural groups. In R. M. Eisler & M. Hersen (Eds.), Handbook of gender, culture, and health (pp. 101–132). New York, NY: Routledge.
Pérez-Escamilla, R. (2009). Dietary quality among Latinos: Is acculturation making us sick? Journal of the American Dietetic Association, 109(6), 988–991.
Read, J. G., & Gorman, B. M. (2010). Gender and health inequality. Annual Review of Sociology, 36, 371–386.
Ricker, P. P., & Bird, C. E. (2005). Rethinking gender differences in health: Why we need to integrate social and biological perspectives. Journals of Gerontology Series B, 60, S40–S47.
Robert Wood Johnson Foundation. (2008). America’s health starts with healthy children: How do states compare? Princeton, NJ: Author.
Szasz, T. S. (2010). The myth of mental illness: Foundations of a theory of personal conduct. New York, NY: Harper Perennial.
Van Cleave, J., Gortmaker, S. L., & Perrin, J. M. (2010). Dynamics of obesity and chronic health conditions among children and youth. JAMA, 303(7), 623–630.
Walker, A. K. (2011, November 20). Where you live can help determine your health, studies say. Bangor Daily News. Retrieved from http://bangordailynews.com/2011/11/20/health/where-you-live-can-help-determine-your-health-studies-say.
Warren, J. R. (2009). Socioeconomic status and health across the life course: A test of the social causation and health selection hypotheses. Social Forces, 87(4), 2125–2153.
Wray, L. A., Herzog, A. R., Willis, R. J., & Wallace, R. B. (1998). The impact of education and heart attack on smoking cessation among middle-aged adults. Journal of Health and Social Behavior, 39, 271–294.
