Main Body
8. Two Main Classes of Receptor Ligands in Pharmacology: Agonists & Antagonists
Agonists: tend to be smaller molecules that effect activation of receptors. 
Note: This may result in stimulation or inhibition of cell and organ function
Full agonists: produces maximal biological response
- Has maximal POSITIVE INTRINSIC activity (EFFICACY)
Partial agonists: produces partial maximal biological response as compared to full agonist
- has lower POSITIVE INTRINSIC activity
- may COMPETITIVELY INHIBIT full agonist preventing maximal biological response
- If the partial agonist is bound to the receptor, the full agonist cannot bind
- may have higher, lower or the same affinity (potency) for the receptor as the full agonist
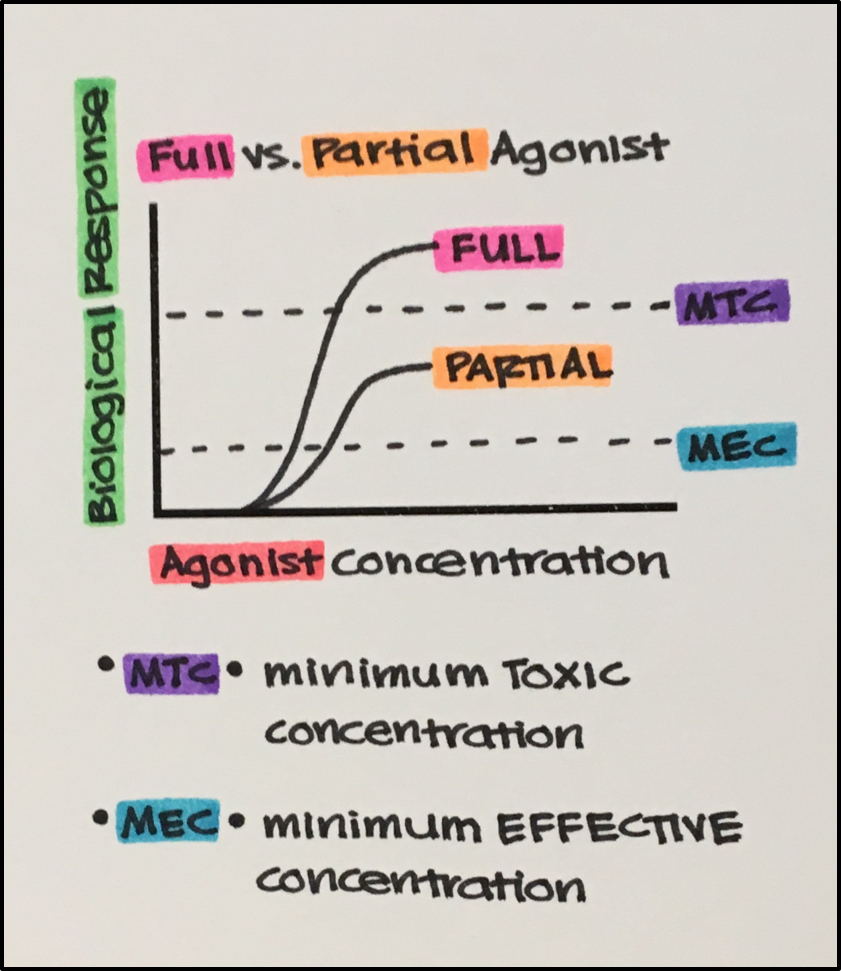
Why use a partial agonist? Full agonist may cause too much activation resulting in toxicity or receptor adaptation on prolonged use (desensitization, downregulation). The lower efficacy of partial agonists minimizes these complications.
Inverse agonists: produces opposite biological response to that of the endogenous agonist/neurotransmitter
- has NEGATIVE INTRINSIC activity (EFFICACY)
Example: GABAA receptor: agonists (benzodiazepines) produce a sedative effect whereas inverse agonists (i.e. Rho15-4513 — originally designed as alcohol antidote) produce anxiety-like effects.
Antagonists: tend to be larger molecules producing INHIBITORY effect. 
- there are antagonists that act at the receptor, also known as receptor antagonists,
**Antagonists DO NOT have INTRINSIC ACTIVITY (EFFICACY): reminder: antagonist simply block the agonist from binding. Furthermore, keep in mind that just because antagonists do not have intrinsic activity does not mean they do not have physiological consequences.
Example: While the beta-1 antagonist DOES NOT have INTRINSIC activity on its own, it still has pharmacological effects in vivo. Under normal circumstances, when a person is exercising norepinephrine is released binds to beta-1 receptors resulting in increased cardiac inotropy (contractility) as well as increased chronotropy (heart rate) to accommodate the increased demand for oxygen. If an individual were using a beta-1 antagonist (a.k.a. beta blocker), it would prevent norepinephrine from binding to beta-1 receptors thus causing reduced contractility and lower heart rate compared to someone who is not using a beta-1 antagonist. Labetalol is an example of a beta-1 antagonist used in individuals who have angina (chest pain) associated with increased heart rate. This drug enables them to exercise, while maintaining a lower heart rate so as to avoid chest pain.
Competitive Antagonist/Inhibitor: REVERSIBLE or SURMMOUNTABLE
-
- Binds to a receptor at the same site as an endogenous or pharmacological agonist, blocking agonist binding and therefore receptor activation.
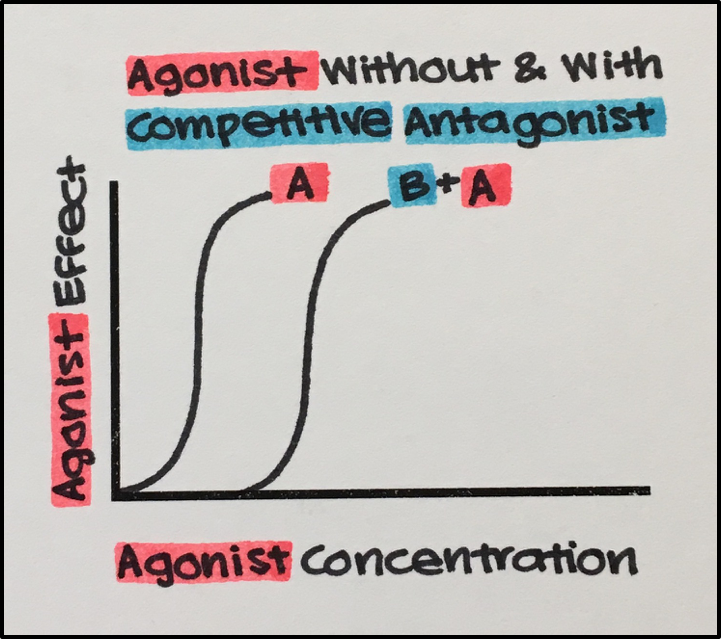
- Antagonism is reversed by increasing the amount/dose of agonist (surmountable). While competitive antagonists do not affect agonist efficacy (maximal response), they do decrease AFFINITY and POTENCY. Thus, a normal maximal response to the agonist may be attained in the presence of a competitive antagonist, albeit at higher agonist concentrations. Thus, agonist dose-response curve is therefore SHIFTED TO THE RIGHT (more agonist needed to produce the same response) in the presence of a competitive antagonist (REFER TO GRAPH).
In this graph:
- A: agonist
- A + B: agonist + competitive antagonist
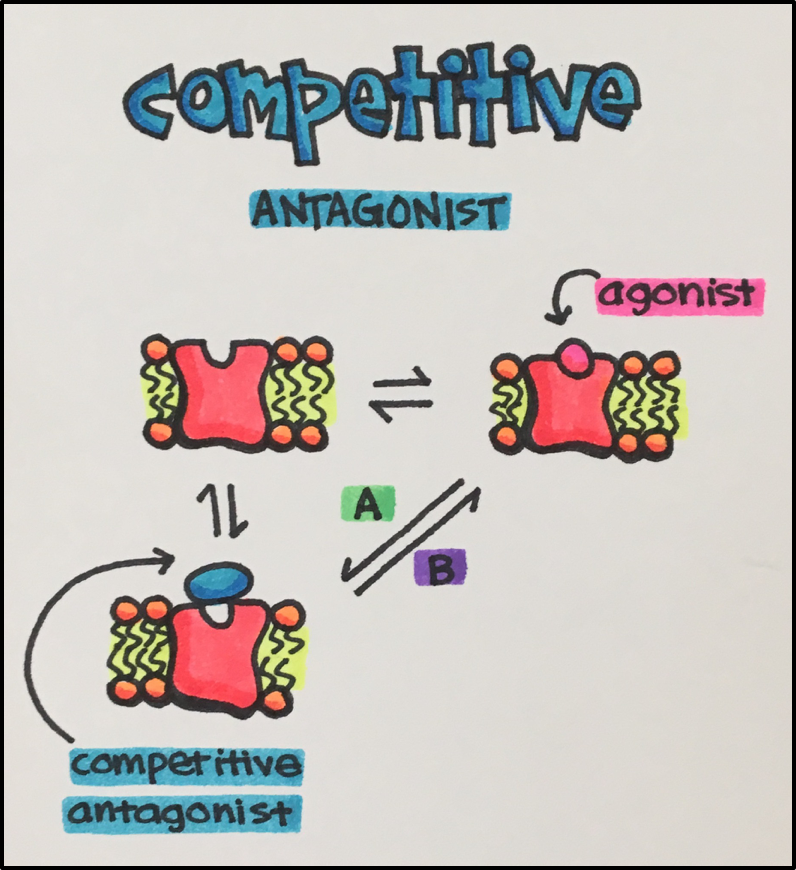
The receptor can interact with the agonist OR the competitive antagonist, but not both, i.e. binding is mutually exclusive.
See above: When the agonist concentration/dose is gradually increased, the equilibrium shifts towards formation of agonist-receptor complex [B]. The opposite is true when the antagonist concentration is increased [A].
- Competitive antagonists have an affinity (potency) for a receptor, however, do not have intrinsic activity: REMINDER: antagonists lack intrinsic activity
Non-Competitive Receptor Antagonists: UNSRUMMOUNTABLE
Two class:
A. IRREVERSIBLE
B. ALLOSTERIC
A. Irreversible Non-Competitive Antagonists:
-
- Usually bind to the same site as the agonist, however, it is not readily displaced like competitive antagonists.
- Generally irreversible due to the formation of a covalent bond between the antagonist and the receptor, in essence reducing the number of receptors available to the agonist.
- In the ABSENCE of SPARE RECEPTORS: The agonist dose-response curve will exhibit a lower maximum that is proportional to the dose of the non-competitive antagoinst.
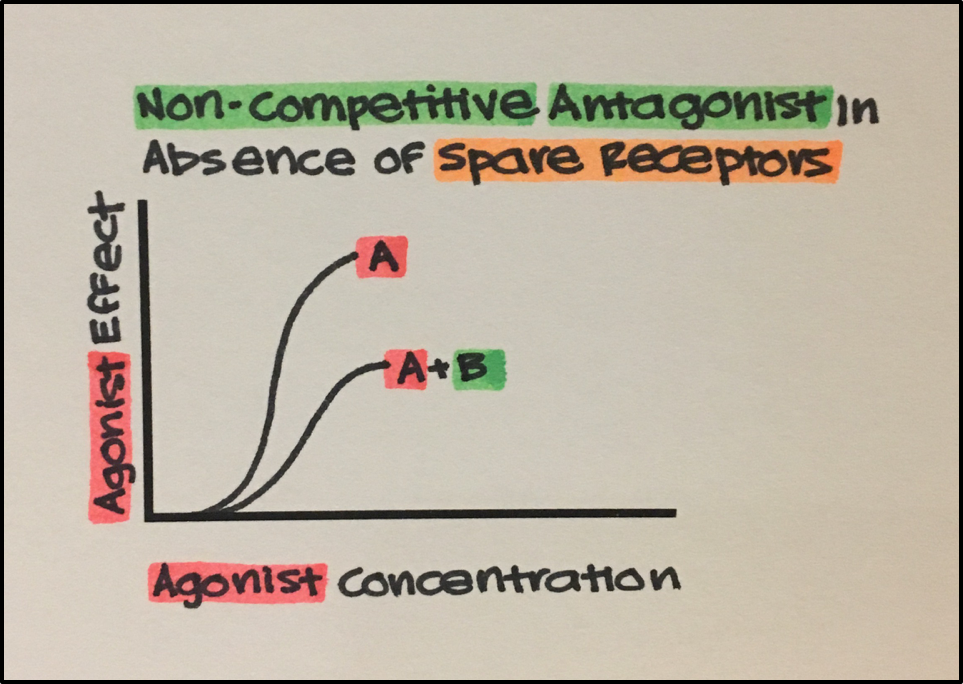
- See above: Unlike competitive antagonists, non-competitive antagonists reduce the actual number of receptors available to be activated, therefore, EFFICACY is REDUCED. The agonist exhibits a lower maximum response in the presence of the non-competitive inhibitor.
- A agonist
- A + B agonist with irreversible non-competitive antagonist
In the presence of spare receptors: Agonist dose-response curve will exhibit unaltered maximal response with increasing doses of the irreversible antagonist, until all spare receptors are exhausted. At this point, higher doses of the antagonist will cause dose-dependent reduction in the maximal response (reduced efficacy).
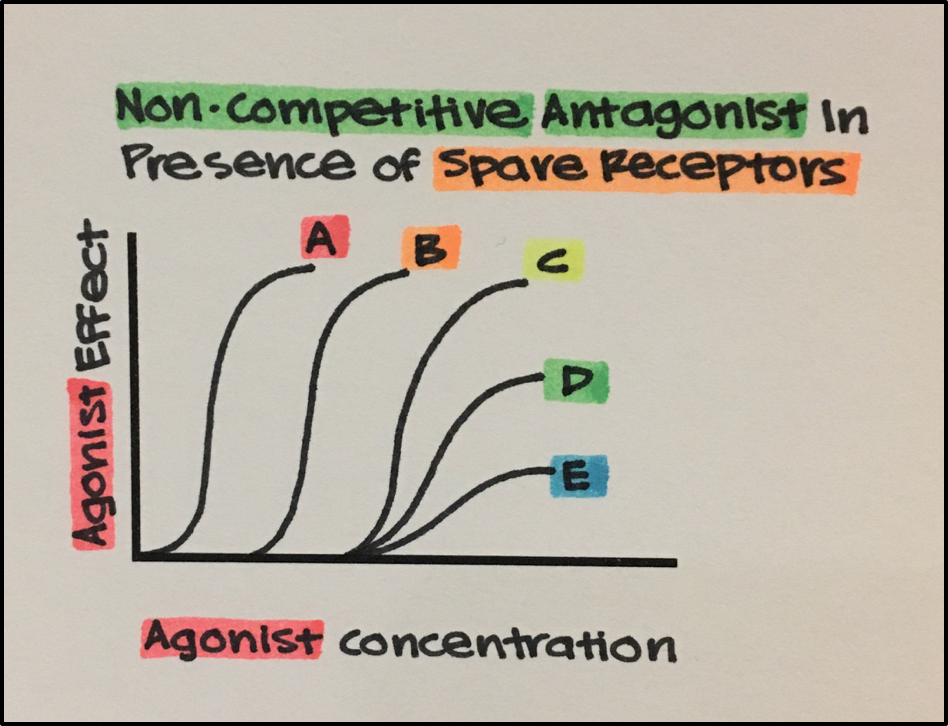
- See above: A, agonist alone exhibits maximal response (efficacy) and affinity (potency) for the receptor. B, agonist plus non-competitive antagonist: the agonist still exhibits maximal response because there are spare receptors, however, its affinity for the receptor is reduced. It is not until D, agonist plus higher concentration of non-competitive antagonist, that the agonist starts to exhibit a lower maximal response as all spare receptors have been eliminated by the irreversible antagonist.
B. Allosteric Non-Competitive Antagonists: A drug may bind to a site (allosteric site) on the receptor different from that where an agonist binds (primary or classical binding site). Binding to the allosteric site modifies the conformation of the primary site. In case of (negative) allosteric antagonists the altered conformation is less responsive to the agonist. Increasing agonist concentration does not displace the allosteric antagonist from the receptors since the two drugs bind to different sites, i.e. this type of antagonism is non-competitive and unsurmountable. See other types of allosteric modulators below.
Physiological Antagonist
- Molecules that do NOT bind the same receptor as the endogenous or a pharmacological agonist, but produce an effect that is opposite to the agonist effect.
Example: epinephrine is a physiological antagonist to histamine, even though they bind to their own specific receptors. When histamine binds to its receptor, arterial pressure decreases through vasodilation. However, when epinephrine binds to its receptor, arterial pressure increases through vasoconstriction, thus counteracting histamine or producing an antihistamine effect.
Chemical Antagonists:
- Drugs that do not interact with the agonist receptor but rather reduce the concentration of an agonist by forming a chemical complex; also known as chelating agents.
Example: Phosphate binders are used to prevent hyperphosphatemia in patients who have chronic kidney disease. Phosphate binders can act as a chemical antagonist with a number of medications including quinolone. Phosphate binders from a complex with quinolone reducing its effectiveness. Patients should be counseled to take a phosphate binder 3 hours before or after taking quinolone.
