21 SA NG Tube Placement
WHY IS SWALLOWING DANGEROUS? quick video describes the act of swallowing can be dangerous if patient does not have a working gag/swallow reflex using a human oral cavity model.
Fluoroscopy of a Dog eating– note the food passing DORSAL to the tracheal opening, the wonder of the laryngeal region!
NG TUBE PLACEMENT Scroll down for NG tube placement in a NUTSHELL, less detail :)… It is all important 🙂
Small Animal-NG tubes often placed in quiet and compliant awake patients, or patients under light sedation.
Large Animal-NG tubes often placed in awake compliant patients-common in horses. You will learn this technique in LAM and LAS.
-
- Place a couple drops of Ophthalmic Proparacaine in nasal passage (BE SUPER CAREFUL TO NOT CONTAMINATE TIP!) *often clinics will keep a separate bottle of ophthalmic proparacaine just for this purpose well labeled in the Fridge! DO THIS FIRST SO IT STARTS WORKING WHILE YOU GET THINGS READY. TIDBIT: can place an additional couple drops of clinic use proparacaine for eyes only into the eye of the same side for additional nasopharyngeal local anesthesia.
- Pick appropriate length and width of tube for size of patient and measure tube to last rib for NG tube to 7-8 rib for NE tube and mark tube with Sharpie (generally not helpful to use tape to mark as impedes gentle movement through sensitive nasal mucosa). Most tubes used today are made especially for feeding cats and dogs, 1) removable guide wire to give some suppleness to the tubes-without are too floppy to pass easily. 2) give helpful size guidelines for size of animal, 3) have handy measuring marks, 4) have weighted tips to ease placement, 5) are radio-dense to show up well on radiographs and 6)come with a cap to secure to the end of the tube prior to removal!. Some can be trimmed, others are one length only. Most cats one can use a 5-8 fr red rubber (larger sizes tend to be a bit stiff, catheter or feeding tube, Dogs dependent on size, especially length, usually are 8-10 fr.
- Lube tube
Lubricating lightly the entire tube is helpful esp. w/cadaver practice-strategize a good way to do this? - Have holder slightly stretch out the head and neck of patient
- Gently push nasal planum dorsal (some times called “piggy nose”)

- 6. Aim the tube ventral and medial to avoid the dorsal meatus and into nasopharynx-oropharynx,
 7. Gently advance tube, (some will sneeze) when close to epiglottis (by eyeballing how much tube is in), have the restrainer direct the nose downward to help direct tube into esophagus.
7. Gently advance tube, (some will sneeze) when close to epiglottis (by eyeballing how much tube is in), have the restrainer direct the nose downward to help direct tube into esophagus.
- Please note the following structures in the photo of an anatomical specimen of half a cat head and neck below; Yellow-Larynx, Blue-Trachea, Red-Esophagus.
- The NG tube tip is right at the epiglottis-this is the point at which the tube could go over the dorsal aspect of the closed epiglottis and into the esophagus (proper placement), OR accidentally be directed between the arytenoid cartilages into the trachea (improper placement).>
- By gently placing nose down as you are feeding the tube, the tube is directed dorsally over the epiglottis and into the esophagus. THIS IS AN IMPORTANT POINT!

Red rubber catheter at the point of either going dorsal over the green epiglottis, or more ventral within the yellow larynx and between the arytenoid cartilages and vocal folds into the trachea! Esophagus outlined in red, trachea outlined in blue 8. Watch for swallow, this takes some practice as can be subtle. Remember the swallow reflect will be subdued in a sedated or moribund patient, and absent in an anesthetized patient-who should have ET tube placed, and of course you wont see this reflex in a cadaver.
- 9. Continue to pass tube until you see the mark at the nose-you may of may not see the tube pass along the left side of the neck (tube is pretty small) DONT force the tube, can instill a bit of air if resistance felt, REMEMBER TO REMOVE THE GUIDEWIRE!
- 10. CONFIRM TUBE PLACEMENT Remember these tests are not accurate in a cadaver!
- Drawing back with syringe on tube- negative pressure indicative of proper placement (however the tube could be in an air pocket! Keep drawing to see if becomes negative pressure?
- Instill a few mls of air and auscultate for bubbling sound on left cranial abdomen-the location of the stomach
- Remember no cough is not a reliable indicator of being in the esophagus/stomach especially if the patient is sedated!
- Also palpate neck you should feel trachea and maybe additionally feel the NG tube (difficult if very small tube),
- Depending on how sedate an animal is you can confirm placement by direct visualization! DO THIS!!
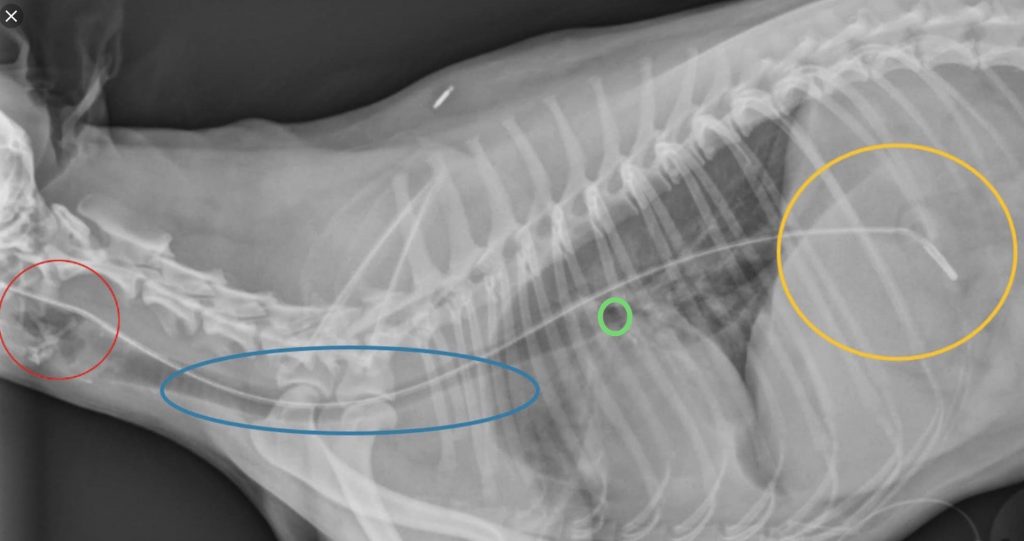
- A V/D or Lateral (required by U of MN VMC in SA patients with NG tube). SEE RADIOGRAPH BELOW
- dorsal to larynx, variable position by thoracic inlet as esophagus overlaps trachea, dorsal to Corina, past diaphragm in stomach
- 11. Secure tube-This is not an objective of this lab, ponder the variations of fixation and ask clinicians you encounter in the future what they prefer and why? Often tube attached at the lateral nasal planum-skin junction, lidocaine gel, thread suture into needle, place needle, pull suture, remove needle, tie knot, then secure to tube using finger trap suture, additional sutures along side of face. Many options! AVOID THE WHISKERS they are very sensitive. Securing is a variable art be open to how SAM/ICU/ECC secures NG tubes as they have a lot of experience! An E-collar is placed to prevent rubbing on tube.
- 12. Removal -some place a drop of Ophthaine in nostril, cut suture, kink tube closed and pull gently and fairly swiftly out, patients often crinkle up nose and may sneeze or cough, and occasionally can have a few drops of blood from irritated nasal mucosa. FINGER ON THE END OF A STRAW TO KEEP FLUID IN STRAW VIDEO
Video of NG tube removal using human oral cavity model demonstration of the importance of having a patient who has a good gag/swallow reflex AND stopper or finger on the end of an NG tube, or kinking an NG tube using human oral cavity model as NG tube pulled out with open epiglottis!
-
- A few things to consider and know before placing an NG tube
- generally you need to feed a prepared liquid diet from a can, or spend some time reasearching liquid diets and how to “departiculate” them as clogs can be common. Even with filtered preparation (what you filter out may be important fiber) clogs can form…
- make sure to pick properly the clients able feed their pets at home with good instructions, demo use of NG tube and have owners actually do all the steps of NG tube feeding in front of the CVT/DVM.
- If owners have any issues, generally these should have a quick recheck with a knowledgable CVT or DVM to sort it out in person vs. over the phone IMO.
- Always reference feeding guidelines and know components of liquid diets designed for NG tube feeding.
-
We’ll go over proper NG tube placement using radiographs in lab. University of Minnesota, VMC requires the radiographic confirmation of NG tube placement for SA patients. Think about what the significance of these 4 anatomical landmarks are in regards to NG tube placement.
NG TUBE IN A NUTSHELL-used to put things in meds/food, take things out air/fluid/ingesta to improve stomach function prevent reflux etc…
-
- Place a couple drops of Ophthalmic Proparacaine in left nostril (often clinics will keep a separate bottle of ophthalmic proparacaine just for this purpose well labeled in the Fridge!)
- Pick appropriate length and width of tube for size of patient
- Measure NG tube to last rib, NE tube to 7-8 th rib & mark w/Sharpie
- Lightly lube entire tube
- Have holder slightly stretch out the head and neck of patient
- Gently push nasal planum dorsal (“piggy nose”)
- Aim the tube ventral and medial to avoid the dorsal meatus and into nasopharynx-oropharynx,
- Gently advance the tube- some will sneeze. When close to epiglottis (by eyeballing how much tube is in), have the restrainer direct the nose downward to help direct the tube dorsal into the esophagus.
- Watch for swallowing, in awake patients.
- Continue to pass tube until you see the mark at the nose-you may or may not see or feel the tube pass along the left side of the neck (tube is pretty small) REMOVE THE GUIDE WIRE!
- CONFIRM TUBE PLACEMENT(Different indicators of tube placement)
- Drawing back with syringe on tube (negative pressure),
- Instill a few mls of air and auscultate for bubbling sound on left cranial abdomen-the location of the stomach.
- If patient is sedated no coughing is not a reliable indicator of appropriate placement!
- Palpate neck for NG tube is generally not helpful as NG tube is so small its is difficult to feel.
- Depending on how sedate an animal is you can confirm placement by direct visualization!
- Ideally take radiograph-either V/D or Lateral (required by U of MN VMC in SA patients with NG tube).
- dorsal to larynx, variable position by thoracic inlet as esophagus overlaps trachea, dorsal to Corina, past diaphragm in stomach
- Secure by suturing to a location that is preferred by the clinician usually side of face. AVOID THE WHISKERS as they are very sensitive. Finger trap suture, several single sutures, sutures through tape attached to tube are all viable options.
- An E-collar is placed to prevent rubbing on the tube.
- Removal-place a drop of Ophthalmic Proparacaine in nostril prior to removal to ease removal
- Cut suture using suture removal scissors
- Place the stopper on the end of the tube or kink tube closed and pull gently and fairly swiftly out, control the end of the tube so it doesn’t flop all over! Patients often crinkle up their nose and may sneeze or cough, and occasionally can have a few drops of blood from irritated nasal mucosa after tube removal