Theme 5: How Do We Control Our Fertility?
5.4 Hormonal Control of Human Reproduction
The human male and female reproductive cycles are controlled by the interaction of hormones from the hypothalamus and anterior pituitary with hormones from reproductive tissues and organs. In both sexes, the hypothalamus monitors and causes the release of hormones from the pituitary gland. When the reproductive hormone is required, the hypothalamus sends a gonadotropin-releasing hormone (GnRH) to the anterior pituitary. This causes the release of follicle stimulating hormone (FSH) and luteinizing hormone (LH) from the anterior pituitary into the blood. Note that the body must reach puberty in order for GnRH to be produced. Although FSH and LH are named after their functions in female reproduction, they are produced in both sexes and play important roles in controlling reproduction. Other hormones have specific functions in the male and female reproductive systems.
*
Male Hormones
At the onset of puberty, the hypothalamus causes the release of FSH and LH into the male system for the first time. FSH enters the testes and stimulates the Sertoli cells to begin facilitating spermatogenesis using negative feedback, as illustrated in Figure 1. LH also enters the testes and stimulates the interstitial cells of Leydig to make and release testosterone into the testes and the blood.
Testosterone, the hormone responsible for the secondary sexual characteristics that develop in the male during adolescence, stimulates spermatogenesis. These secondary sex characteristics include a deepening of the voice, the growth of facial, axillary, and pubic hair, and the beginnings of the sex drive.
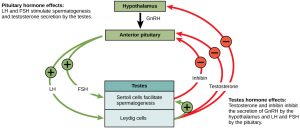
A negative feedback system occurs in the male with rising levels of testosterone acting on the hypothalamus and anterior pituitary to inhibit the release of GnRH, FSH, and LH. This system works to keep the concentration of testosterone in the blood at a relatively constant level in each male individual after puberty. If testosterone levels become elevated above their normal levels (called the set point levels), the testosterone will inhibit the hypothalamus from secreting as much GnRH. This will in turn cause lower levels of FSH and LH to be produced. Lower LH levels will lower the amount of stimulation that the Leydig cells receive, and lower the production of testosterone. The Sertoli cells also produce the hormone inhibin, which is released into the blood when the sperm count is too high. This inhibits the release of GnRH and FSH, which will cause spermatogenesis to slow down. If the sperm count reaches 20 million/ml, the Sertoli cells cease the release of inhibin, and the sperm count increases.
Conversely, if testosterone levels are decreased, there will be less inhibition of GnRH production by the hypothalamus. This will cause more stimulation of the anterior pituitary, increased FSH and LH secretion, and increased stimulation of the Leydig cells and Sertoli cells. The end result will be an increase in testosterone levels. As you may imagine, this intricate system of regulation is constantly responding to slight fluctuations in testosterone with concomitant fluctuations in hypothalamic secretion of GnRH, and anterior pituitary secretion of FSH and LH.
*
Female Hormones
The control of reproduction in females is more complex. As with the male, the anterior pituitary cause the releases the hormones FSH and LH. GnRH controls the secretion of FSH and LH, but in a more complex cyclical manner. In addition, estrogens and progesterone are released from the developing follicles. In females, FSH stimulates development of egg cells, called ova, which develop in structures called follicles. Follicle cells produce the hormone inhibin, which inhibits FSH production. LH also plays a role in the development of ova, induction of ovulation, and stimulation of estrogen and progesterone production by the ovaries. Estrogen and progesterone are steroid hormones that prepare the body for pregnancy. Estrogen produces secondary sex characteristics in females, including breast development, maturation of the external genitalia, and widening of the hips, while both estrogen and progesterone regulate the menstrual cycle.
The Ovarian Cycle and the Uterine Cycle
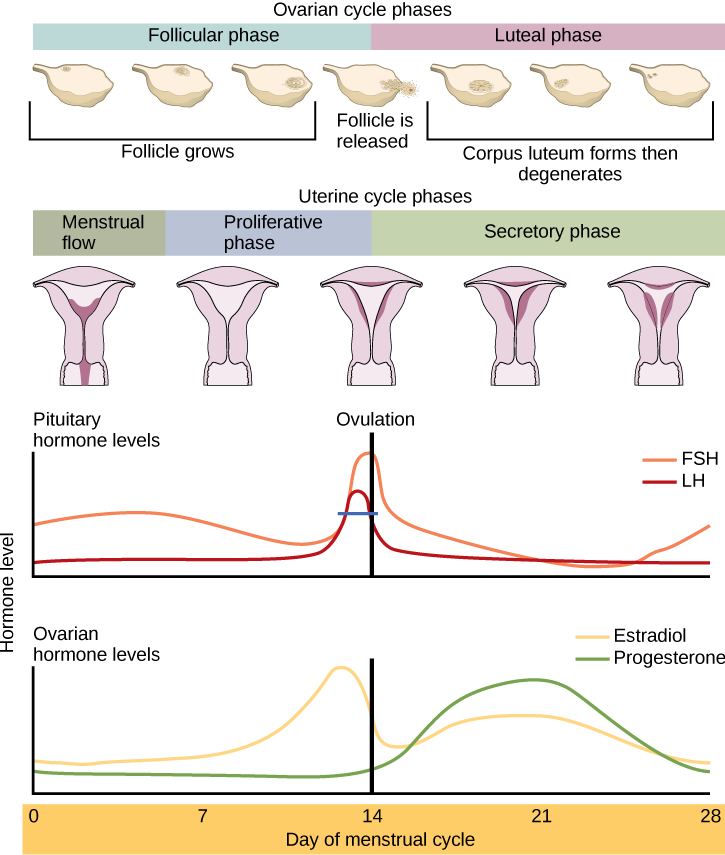
Female reproduction occurs in a cyclical fashion in females. The ovarian cycle governs the preparation of endocrine tissues and release of eggs, while the uterine cycle governs the preparation and maintenance of the uterine lining to receive any potential fertilized eggs. The uterine cycle is sometimes referred to as the menstrual cycle. These cycles occur concurrently and are coordinated over a 22–32 day cycle, with an average length of 28 days. The events of these cycles and the hormone actions during them are summarized in Figure 2.
The timing of the uterine cycle starts with the first day of menses, referred to as day one of a females’s period. Cycle length is determined by counting the days between the onset of bleeding in two subsequent cycles. Because the average length of a female’s uterine cycle is 28 days, this is the time period used to identify the timing of events in the cycle. However, the length of the uterine cycle varies among women, and even in the same woman from one cycle to the next. The menses phase of the uterine cycle is the phase during which the lining is shed; that is, the days that the woman menstruates. Although it averages approximately five days, the menses phase can last from 2 to 7 days, or longer. FSH, LH and progesterone levels are low at this time; the drop in these levels causes the endometrial lining to shed.
Once menstrual flow ceases, the endometrium begins to proliferate again, marking the beginning of the proliferative phase of the menstrual cycle. This usually occurs at around day 5-7 of the cycle. The proliferative phase is named after the growth, or proliferation of the endometrium during this phase, which is caused by increasing concentrations of estrogen.
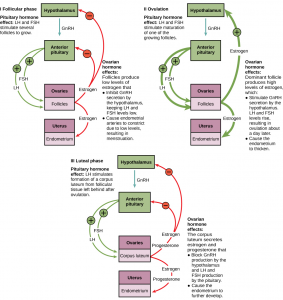
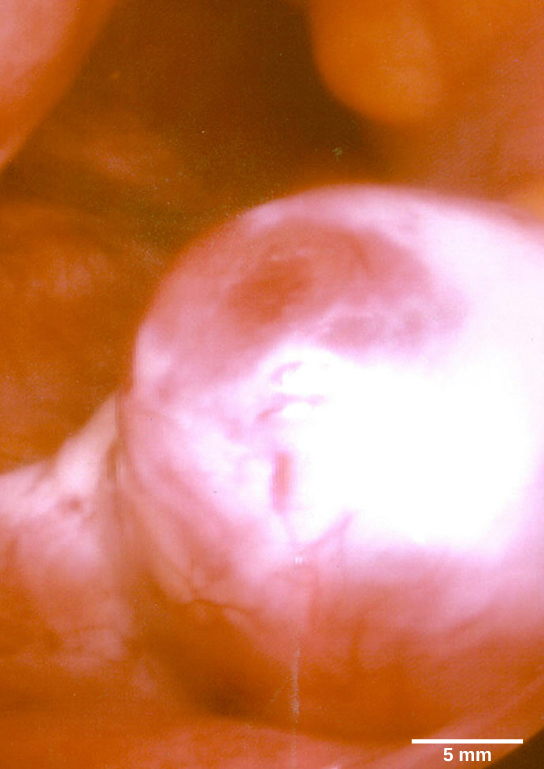
The first half of the ovarian cycle is the follicular phase, which occurs on day 1-14 of the cycle, overlapping with both menses and the proliferative phase of the uterine cycle. Slowly rising levels of FSH and LH cause the growth of follicles on the surface of the ovary. This process prepares the egg for ovulation. As the follicles grow, they begin releasing estrogens and a low level of progesterone. Just prior to the middle of the cycle (approximately day 14), the high level of estrogen causes FSH and especially LH to rise rapidly, then fall. The spike in LH causes ovulation: the most mature follicle, like that shown in Figure 3, ruptures and releases its egg. The follicles that did not rupture degenerate and their eggs are lost. The level of estrogen decreases when the extra follicles degenerate.
Following ovulation, the ovarian cycle enters its luteal phase, illustrated in Figure 2, and the menstrual cycle enters its secretory phase, both of which run from about day 15 to 28. The luteal and secretory phases refer to changes in the ruptured follicle. The cells in the follicle undergo physical changes and produce a structure called a corpus luteum. The corpus luteum produces estrogen and progesterone. The progesterone facilitates the maintenance and further development of the uterine lining and inhibits the release of further FSH and LH. The uterus is being prepared to accept a fertilized egg, should it occur during this cycle. The inhibition of FSH and LH prevents any further eggs and follicles from developing, while the progesterone is elevated. The level of estrogen produced by the corpus luteum increases to a steady level for the next few days.
If no fertilized egg is implanted into the uterus, the corpus luteum degenerates and the levels of estrogen and progesterone decrease. The endometrium begins to degenerate as the progesterone levels drop, initiating the next menstrual cycle. The decrease in progesterone also results in increased FSH and LH secretion from the anterior pituitary, and starts the cycles again. Figure 4 visually compares the ovarian and uterine cycles as well as the commensurate hormone levels.
Menopause
As women approach their mid-40s to mid-50s, their ovaries begin to lose their sensitivity to FSH and LH. Menstrual periods become less frequent and finally cease; this is menopause. There are still eggs and potential follicles on the ovaries, but without the stimulation of FSH and LH, they will not produce a viable egg to be released. The outcome of this is the inability to have children.
The side effects of menopause include hot flashes, heavy sweating (especially at night), headaches, some hair loss, muscle pain, vaginal dryness, insomnia, depression, weight gain, and mood swings. Estrogen is involved in calcium metabolism and, without it, blood levels of calcium decrease. To replenish the blood, calcium is lost from bone which may decrease the bone density and lead to osteoporosis. Supplementation of estrogen in the form of hormone replacement therapy (HRT) can prevent bone loss, but the therapy can have negative side effects. While HRT is thought to give some protection from colon cancer, osteoporosis, heart disease, macular degeneration, and possibly depression, its negative side effects include increased risk of: stroke or heart attack, blood clots, breast cancer, ovarian cancer, endometrial cancer, gall bladder disease, and possibly dementia.
Reproductive Endocrinologist
A reproductive endocrinologist is a physician who treats a variety of hormonal disorders related to reproduction and infertility in both men and women. The disorders include menstrual problems, infertility, pregnancy loss, sexual dysfunction, and menopause. Doctors may use fertility drugs, surgery, or assisted reproductive techniques (ART) in their therapy. ART involves the use of procedures to manipulate the egg or sperm to facilitate reproduction, such as in vitro fertilization.
Reproductive endocrinologists undergo extensive medical training, first in a four-year residency in obstetrics and gynecology, then in a three-year fellowship in reproductive endocrinology. To be board certified in this area, the physician must pass written and oral exams in both areas.
Section Summary
The male and female reproductive cycles are controlled by hormones released from the hypothalamus and anterior pituitary as well as hormones from reproductive tissues and organs. The hypothalamus monitors the need for the FSH and LH hormones made and released from the anterior pituitary. FSH and LH affect reproductive structures to cause the formation of sperm and the preparation of eggs for release and possible fertilization. In the male, FSH and LH stimulate Sertoli cells and interstitial cells of Leydig in the testes to facilitate sperm production. The Leydig cells produce testosterone, which also is responsible for the secondary sexual characteristics of males. In females, FSH and LH cause estrogen and progesterone to be produced. They regulate the female reproductive system which is divided into the ovarian cycle and the menstrual cycle. Menopause occurs when the ovaries lose their sensitivity to FSH and LH and the female reproductive cycles slow to a stop.
*
Glossary
- estrogen
- reproductive hormone in females that assists in endometrial regrowth, ovulation, and calcium absorption
- follicle stimulating hormone (FSH)
- reproductive hormone that causes sperm production in men and follicle development in women
- gonadotropin-releasing hormone (GnRH)
- hormone from the hypothalamus that causes the release of FSH and LH from the anterior pituitary
- inhibin
- hormone made by Sertoli cells; provides negative feedback to hypothalamus in control of FSH and GnRH release
- interstitial cell of Leydig
- cell in seminiferous tubules that makes testosterone
- luteinizing hormone (LH)
- reproductive hormone in both men and women, causes testosterone production in men and ovulation and lactation in women
- menopause
- loss of reproductive capacity in women due to decreased sensitivity of the ovaries to FSH and LH
- ovarian cycle
- cycle of preparation of egg for ovulation and the conversion of the follicle to the corpus luteum
- ovulation
- release of the egg by the most mature follicle
- progesterone
- reproductive hormone in women; assists in endometrial re-growth and inhibition of FSH and LH release
- Sertoli cell
- cell in seminiferous tubules that assists developing sperm and makes inhibin
- testosterone
- reproductive hormone in men that assists in sperm production and promoting secondary sexual characteristics
-
- uterine cycle
- cycle of the degradation and re-growth of the endometrium; also called the menstrual cycle
