13. Anal Sac Disorders
Learning Objectives
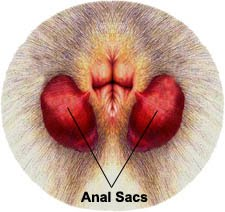
- Know! Anal sac disorders are primarily associated with one of four conditions: impaction, inflammation/infection, abscessation or neoplasia. Anal sacs can be palpated on either side of the anal canal at about 4 and 8 o’clock positions.
- Know! The clinical signs of impacted or inflamed/infected anal sacs are similar and include scooting and licking or biting at the perianal area. However, these signs are not specific and can occur with many others dermatological diseases.
- Know! Abscessed sacs will often rupture and cause cellulitis of the surrounding tissue, which will present erythema and swollenness of the affected area and eventually the development of sinus tracts.
- Know the macroscopic characteristic of a normal anal sacs’ content.
- Know the macroscopic characteristic of the content of anal sacs in cases of impaction or inflammation/infection.
- Remember! It is difficult to differentiate the microscopic characteristic of a normal anal sac content from an inflamed/infected content because normal content also contains neutrophils and bacteria, which can also be intracellular. Criteria that have been used, but are not validated yet, include the presence of more than 10% of the microscopic fields (100X) with intracellular bacteria and red blood cells.
- Know! Anal sac tumors are uncommon. The most common one is apocrine gland adenocarcinoma of anal sac (AGASAC). Affected animals may present paraneoplastic hypercalcemia and have polyuria and polydipsia. Metastasis to regional lymph nodes occurs frequently but the neoplasm can also metastasize to the lungs. Clinically, a firm mass with or without ulceration will be present in the areas of the anal sacs (4 and 8 o’clock positions). However, the mass can be very small and only palpated via careful rectal examination.
- Know! Diagnosis of anal sac diseases should include the patient’s history, suggestive clinical signs, manual expression and macroscopic characterization of the anal sac content, and direct microscopic evaluation (i.e. cytology) of the anal sac content. Fine need aspiration and biopsy should be performed in the presence of perianal/perineal masses or masses associated with the sacs. In cases of AGASAC, imaging of the thorax and abdomen should be performed.
- Know! The management of inflammation/infection of anal sacs (i.e. anal sacculitis) include gentle expression, flushing with saline multiple times until the sac content comes out clean, and local administration of an ointment containing antimicrobials (antibiotic ± antifungal) and a glucocorticoid to reduce the inflammation. Repeat the procedure every 2 to 3 weeks until the anal sacculitis is resolved. We only recommend systemic antibiotic therapy in cases of cellulitis. Select the antibiotic based on culture and susceptibility.
- Remember! Consult with or refer to an oncologist for appropriate management of anal sac neoplasia.
-
General Considerations
-
- The anal sacs of dogs and cats are paired structures located between the muscles of the internal and external anal sphincters at about 4 and 8 o’clock positions. In dogs, they open at the mucocutaneous junction of the anus, and in cats at a prominence located about 0.25 cm lateral to the anus. The sacs of dogs and cats are lined by thin stratified squamous epithelium. Sebaceous glands line the neck of the anal sacs, while apocrine glands line the fundus. The content of the sacs is usually expressed passively during defecation, but they can also be actively expressed via contraction of the internal and external anal sphincters.
-
-
- Reported incidences of non-neoplastic anal sac diseases in dogs range from 1.5% to 12.5%. These cases were diagnosed in general practice and referral institutions from many parts of the world, which can explain the broad range. The incidence in cats has not been reported but it is believed that cats are less affected by non-neoplastic anal sacs diseases than dogs.
- Factors considered to have an impact in the development of anal sac diseases include stool quality, diet type, body condition score, skin disease, and breed.
- The pathogenesis of inflammatory anal sac disease is not fully understood. It is speculated that an initial anal sac impaction occurs followed by bacterial overgrowth, which ultimately leads to a local inflammatory reaction.
Important Facts
- Factors considered to have an impact in the development of anal sac diseases include stool quality, diet type, body condition score, skin disease, and breed.
- It is speculated that the pathogenesis of inflammatory anal sac disease involves an initial anal sac impaction, which leads to bacterial overgrowth and ultimately a local inflammatory reaction.
-
Anal Sac Diseases and Clinical Signs
- Primary anal sac disease is classically divided into four clinical entities as described below. Except for neoplasia, these disorders are considered a continuum and differentiation between them is poorly defined.
- Impaction – It is a common anal sac problem of dogs, but it is rare in cats. There is no sex or age predilection; however, it appears to occur more often in small breeds and obese dogs. Overfilling and distention of the anal sac may be due to inflammatory bowel disease, diarrhea, obesity, change in the character of the secretion, excess glandular secretion, or change in the anal sphincters muscle tone. Clinical signs subside after expression of the impacted content, but relapses are common.
- Inflammation/infection – It is believed to occur because of chronic or recurrent impaction. Other suggested reasons include fecal contamination, obesity, low tail carriage and chronic intestinal diseases. Neutrophils and intracellular and extracellular (more often) bacteria are found in the contents of normal anal sacs making it difficult to separate an infected from a normal sac based on cytological examination. Criteria that have been used, but not validated in studies, are the presence of more than 10% of the microscopic fields (100x) showing intracellular bacteria and red blood cells. Moreover, the presence of blood and pus in the anal sac content and suggestive clinical signs support a diagnosis of anal sacculitis.
- Abscessation – It occurs because of chronic infection associated with some degree of impaction. The sac eventually ruptures, and its content extends to the peripheral tissue resulting in cellulitis and ultimately fistulation.
- Neoplasia – The most common neoplasia of dogs is apocrine gland anal sac adenocarcinoma (AGASAC), which often metastasizes to regional lymph nodes but can also spread to the lungs and other internal organs. English cocker spaniel was overrepresented in one study. Dogs may have paraneoplastic hypercalcemia and associated polyuria and polydipsia. AGASAC is uncommon in cats. Squamous cell carcinoma has also been reported in dogs and cats, and melanoma, papillary cystadenoma, soft tissue sarcoma combined with AGASACA and mast cell tumor in dogs. A mass or swelling in the perianal area and tenesmus and constipation may be present but some tumors may only be diagnosed via rectal palpation.
- Clinical signs
- Signs of anal sac impaction and inflammation/infection are similar and include scooting and licking or biting at the anus and perianal region. These signs, however, are not pathognomonic and can be seen with atopic dermatitis, food allergy, perivulvar dermatitis, psychogenic anal licking, tail fold dermatitis, and perianal fistulas.
- Primary anal sac disease is classically divided into four clinical entities as described below. Except for neoplasia, these disorders are considered a continuum and differentiation between them is poorly defined.

-
-
- In cases of cellulitis due to abscessation and rupture of the anal sac, perianal swelling, erythema and eventually the formation of sinus tracts will be seen. Pain is present in those cases and typically, only one anal sac is involved. Affected animals are often pyrexic and lethargic.
-

-
-
- Anal sacs with thicken walls and/or distension due to any of the mentioned causes can be palpated on either side of the anal canal at about 4 and 8 o’clock positions.
- The normal anal sac content of dogs and cats is described as pale yellow or straw-colored, serous, clear to translucent, slightly viscous, granular and often having small brownish flecks. A pungent odor is characteristic.
- The abnormal content color varies from greenish yellow (pus) to red (blood) to brown to clay to black.
- Infected anal sacs often are associated with an opaque, thick, red or yellowish/ greenish-colored material, which have a fetid odor.
- Impacted anal sacs are typically characterized by clay- or black-colored contents that are dry or pasty and have minimal odor. The thick and pasty content often has a ribbon-like pattern when expressed.
-

Important Facts
- Primary anal sac disease is divided into four clinical entities: impaction, inflammation/infection, abscessation and neoplasia.
- An abnormally distended and/or thickened anal sacs, due to any cause, can be palpated on either side of the anal canal at about 4 and 8 o’clock positions.
- Clinical signs of impaction and inflammation/infection are similar and include scooting and licking or biting the perianal area. These signs can also occur with many other diseases.
- Abscessation of a chronically infected and impacted sac can result in wall rupturing leading to cellulitis of the surrounding tissue characterized by diffuse swelling, erythema and pain in the perianal region and eventually fistulation. Affected animals can be pyrexic and lethargic.
- The most common anal sac neoplasia of dogs is apocrine gland anal sac adenocarcinoma (AGASAC), which often metastasizes to the lungs and peripheral lymph nodes.
- Normal anal sac content of dogs and cats is described as pale yellow or straw-colored, serous, clear to translucent, slightly viscous, granular, and often having small brownish flecks. A pungent odor is characteristic.
- Abnormal content color varies from greenish yellow (pus) to red (blood) to brown to clay to black color. The consistency varies according to the cause, being typically thick and dry or pasty in cases of impaction.
-
Diagnosis
- The diagnosis is based on the pet’s history, suggestive clinical signs, careful rectal palpation of the anal sacs, and macroscopic and microscopic examination of the anal sacs content.
- In cases of impaction, the sacs will feel firm and enlarged and the content may be difficult to express.
- In cases of abscessation, the anal sac itself and the surrounding tissue are very painful, and sedation may be required for a thorough and proper examination of the patient.
- Macroscopic findings highly suggestive of inflammation/infection are the presence of blood and pus. In cases of impaction, the content is tick, dry to pasty and has a tubular to ribbon-like shape.
- The microscopic exam of normal anal sac content reveals epithelial cells, a few neutrophils and bacteria (typically extracellular). Many leukocytes, red blood cells and numerous bacteria, especially intracellular, indicate diseased anal sacs. However, as mentioned before, criteria that can be used to differentiate normal from infected anal sacs are the presence of more than 10% of the microscopic fields (100x) with intracellular bacteria and red blood cells. These criteria need to be validated in studies.
- Bacterial culture and susceptibility should be performed to select the systemic antibiotic to treat cellulitis.
- In the presence of a mass, fine-needle aspiration and/or biopsy should be performed to rule out neoplasia.
- Imaging of the abdomen and thorax is indicated in cases of AGASAC.
- The diagnosis is based on the pet’s history, suggestive clinical signs, careful rectal palpation of the anal sacs, and macroscopic and microscopic examination of the anal sacs content.
Important Facts
- The diagnosis of anal sac diseases should be based on the pet’s history, suggestive clinical signs, careful rectal palpation of the sacs, and the macroscopic and microscopic examination of the anal sacs content.
- Macroscopic appearance of anal sac content highly suggestive of inflammation/infection is the presence of blood and pus.
- In cases of impaction, the content is tick, dry to pasty and has a tubular to ribbon-like shape.
- In cases of abscessation, the anal sac itself and the surrounding tissue are very painful, and sedation may be required for a thorough and proper examination of the patient.
- Microscopic examination of the anal sacs content showing large number of leukocytes, red blood cells and numerous bacteria, especially intracellular, indicates diseased anal sacs. However, criteria that can be used to differentiate normal from infected sacs are the presence of more than 10% of the microscopic fields (100x) with intracellular bacteria and red blood cells. These criteria need to be validated in studies.
- In the presence of a mass, fine-needle aspiration and/or biopsy should be performed to rule out neoplasia.
- Bacterial culture and susceptibility should be performed to select the systemic antibiotic to treat cellulitis.
- Thoracic and abdominal imaging should be performed in AGASAC cases.
-
Treatment
- Impaction:
- Gentle expression of the anal sacs content is mandatory. In cases where the content is hard to express, a ceruminolytic agent can be instilled into the sacs to help soften the content and allow its adequate removal.
- Feline anal sac impaction typically occurs without infection and may not recur after expression for a long period. In contrast, in dogs, impaction may recur in 19% to 80% of the cases within 3 days to 3 weeks after expression.
- To reduce the frequency of recurrences, regular manual expression for a period of time and diet changes may be beneficial.
- Surgical removal, if frequent recurrences, is an option to offer owners.
- Look for concomitant dermatoses and treat them appropriately.
- Inflammation/Infection:
- Treat locally as follows:
- Express gently the anal sacs content using a gloved, lubricated finger.
- Cut a Tom Cat catheter [3.5 French x 51/2 inch (14 cm)] approximately in half at a right angle. Lubricate the catheter and flush the sacs with saline by gently inserting the catheter into the anal sac opening and through the anal sac duct. Thereafter, attach a 6 mL syringe to the catheter and flush the anal sac until the content comes out clean.
- Instill an ointment or solution containing an antimicrobial and a glucocorticoid into the sacs until the product overflows. The authors typically use ear ointments that contains an antibiotic, antifungal and glucocorticoid.
- Repeat the procedure every 2 to 3 weeks until the sacculitis is resolved. In general, at least three local treatments are needed.
- Sedation is recommended to facilitate the procedure.
- The authors do not recommend using systemic antibiotic to treat anal sacculitis because it is not an effective treatment. In contrast, local treatment is very effective because the concentration of antimicrobials at the site of infection is significantly higher than the MIC needed to inhibit the bacteria.
- Surgical removal, if frequent recurrences, is an option to offer owners.
- Look for concomitant dermatoses and treat them appropriately.
- Treat locally as follows:
- Abscessation:
- If the abscess is not ruptured, hot pack the affected area several times a day until the abscess is ready for drainage.
- The abscess then is lanced and the content thoroughly expressed.
- The anal sac duct must be open, often requiring cannulation.
- When the abscess has ruptured or has been surgically opened, it should be flushed with 10% povidone iodine, diluted hydrogen peroxide and/or chlorhexidine daily until closed.
- In cases of cellulitis, systemic antibiotic therapy should be administered based on culture and susceptibility.
- If the tissue does not heal with medical therapy, surgical excision of the anal sac is indicated.
- Look for concomitant dermatoses and treat them appropriately.
- Neoplasia:
- Consult with or refer to an oncologist for appropriate treatment.
- Impaction:
Important Facts
- Gentle expression of the anal sacs via rectal palpation is indicated in all cases of anal sac impaction or inflammation/infection.
- In some cases of anal sac impaction, a ceruminolytic agent can be instilled into the sacs to help soften the content and allow its adequate removal.
- Treat locally anal sac inflammation/infection by (i) expressing the anal sac content carefully, (ii) flushing the sacs with saline until the contents come out clean, and (iii) infusing the sacs with an ointment or solution containing an antibiotic, a glucocorticoid and/or an antifungal. Repeat the procedure every 2 to 3 weeks, until the sacculitis is resolved.
- Systemic antibiotic therapy based on culture and susceptibility is typically needed in cases of cellulitis.
- Surgical excision may be required for recurrent cases or cases that do not respond to therapy.
- Consult with or refer to an oncologist for appropriate treatment of anal sac neoplasms.
References
Bloom P. Anal sacculitis refractory to standard treatment. Vet Med 2011; 106:122.
Corbee RJ, Woldring HH, van den Eijnde LM et al. A cross-sectional study on canine and feline anal sac disease. Animals 2022; 12:95.
Ehrenzweig J. Novel fiber-rich supplement effective for prevention and treatment of acute, episodic and chronic anal gland disease in dogs and cats. Int J Vet Anim Med 2018; 1:104.
Frankel JL, Scott DW, Erb HN. Gross and cytological characteristics of normal feline anal-sac secretions. J Feline Med Surg 2008; 10:319-323.
Greer W, Calhoun M. Anal sacs of the cat (felis domesticus). Am J Vet Res 1966; 27:773.
James DJ, Griffin CE, Polissar NL et al. Comparison of anal sac cytological findings and behaviour in clinically normal dogs and those affected with anal sac disease. Vet Dermatol 2011; 22:80–87.
Kopke MA, Gal A, Piripi SA et al. Squamous cell carcinoma of the anal sac in two cats. J Small Anim Pract 2020; DOI: 10.1111/jsap.13217
Lake AM, Scott DW, Miller WH Jr, et al. Gross and cytological characteristics of normal canine anal-sac secretions. J Vet Med A Physiol Pathol Clin Med 2004; 51:249-253.
Lundberg A, Koch SN and Torres SMF. Local treatment for canine anal sacculitis: A retrospective study of 33 dogs. Vet Dermatol 2022; DOI: 10.1111/vde.13102.
Miller WH, Griffin GE, Campbell KL. Muller & Kirk Small Animal Dermatology. 7th edn. St Louis: Elsevier Inc., 2013; 708-709.
Montagna W, Parks H. A histological study of the glands of the anal sac of the dog. Anat Rec 1948; 100:297.
O’Neill DG, Hendricks A, Phillips JA et al. Non-neoplastic anal sac disorders in UK dogs: Epidemiology and management aspects of a research-neglected syndrome. Vet Rec 2021; 189:e203.
Robson D, Burton G, Lorimer M. Cytological examination and physical characteristics of the anal sacs of the anal sacs in 17 clinically normal dogs. Aust Vet J 2003; 81:36-41.
Pappalardo E, Martino PA, Noli C. Macroscopic, cytological and bacteriological evaluation of anal sac content in normal dogs and in dogs with selected dermatological diseases. Vet Dermatol 2002; 13:315-322.
Paterson S and Steen S. Anal sacs: a new approach to an old problem? Vet Pract 2016; 31-33.
Shoieb AM and Hanshaw DM. Anal sac gland carcinoma in 64 cats in the United Kingdom (1995-2007). Vet Pathol 2009; 46: 677-683.
Williams LE, Gliatto JM, Dodge RK, et al. Veterinary Cooperative Oncology Group: Carcinoma of the apocrine glands of the anal sac in dogs: 113 cases (1985-1995). J Am Vet Med Asoc 2003; 223:825-831.
