2.8 Generalized Discoid Lupus Erythematosus
-
General Considerations
- Generalized discoid lupus erythematosus is a rare chronic generalized form of discoid lupus erythematosus recently recognized in dogs.
- It is usually not associated with systemic signs.
- Pruritus or pain may rarely be present.
Important Facts
- Generalized discoid lupus erythematosus is a rare chronic generalized form of discoid lupus erythematosus reported in dogs.
- Dogs are usually healthy with only skin involvement.
-
Clinical Signs
- Signalment: Information is based on a review of 10 cases.
- It can affect different breed such as, the hairless Chinese crested dog, shit-tzu, Labrador retriever, miniature pincher, Leonberger, and the toy poodle. It has also been reported in a crossbred dog.
- It appears to affect middle aged to older dogs at about 5 to 12 years of age; median 9 years.
- The female to male ration is 1.0.
- Lesions:
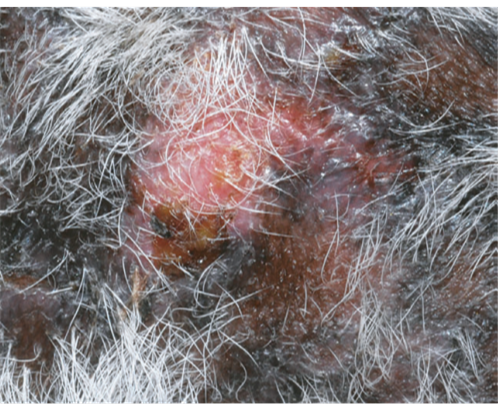
- Multiple well-demarcated annular to polycyclic, hyperpigmented and erythematous plaques, macules and papules. Adherent scaling, crusts, erythema, erosions, ulcers, and hypopigmented atrophic scars may be present. A pattern of reticulated hyperpigmentation can be seen in some dogs.
- Signalment: Information is based on a review of 10 cases.



-
-
- Lesions may be exacerbated by sunlight.
- Distribution:
- Lesions are most often localized to the neck, trunk, and extremities without facial involvement but the face can be affected in some cases. Plaque-type lesion affecting the genital mucocutaneous junctions was reported in few cases.
- Four of 10 cases in a review had plaque lesions at the mucocutaneous junctions of the genitalia.
-

Important Facts
- Generalized discoid lupus erythematosus can affect many breeds.
- The disease typically develops in middle aged to older dogs at 5 to 12 years of age.
- There is no sex predilection.
- Multiple annular to polycyclic, hyperpigmented and erythematous plaques, macules and papules are characteristic lesions.
- Lesions are most commonly localized to the neck, trunk and extremities without facial involvement.
-
Diagnosis
- Differential diagnoses:
- Generalized ischemic dermatopathies (typically vaccine induced), and hyperkeratoric erythema multiforme.
- Compatible history and clinical signs are important components of the diagnostic equation.
- Cytology:
- No acantholytic keratinocytes are present.
- Histopathology:
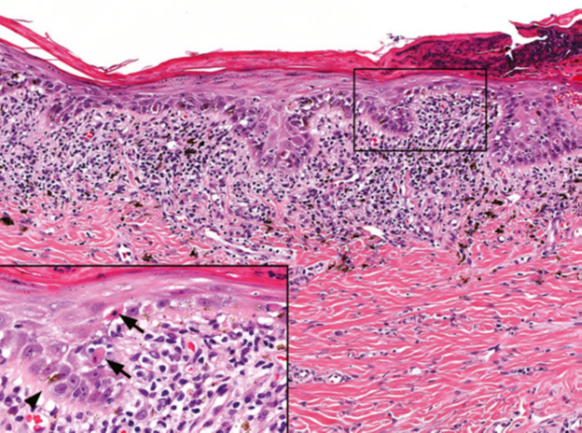
- Interface dermatitis characterized by hydropic-vacuolar changes at the basement membrane zone and basal cell layer is a prominent feature. Apoptosis, with or without lymphocytic satellitosis, is typically present at the basal cell layer but it can also be noticed at the above layers, which can lead to the erroneous diagnosis of erythema multiforme. Lymphocytic interface folliculitis involving the infundibulum and isthmus has also been reported. Pigmentary incontinence can be significant in some areas.
- Select non-ulcerated plaques, macules, and papules to biopsy.
- Differential diagnoses:
-
- Direct immunofluorescence or immunohistochemistry:
- These tests are not routinely performed because more studies need to be done to document their diagnostic value and they are not widely available.
- Deposition of immunoglobulin or complement at the basement membrane zone resulting in staining at the dermal-epidermal junction. This was noted in 90% of the dogs in a case series.
- Remember! Do not rule out generalized discoid lupus erythematosus if the results are negative.
- Preserve samples in Michel’s solution for immunofluorescence and formalin for immunohistochemistry.
- Antinuclear antibody (ANA) test:
- Low titer or negative. It can be performed to investigate coexisting systemic lupus erythematosus if systemic signs are present. However, no progression to systemic lupus erythematosus has been reported in dogs. Moreover, it is important to remember that this test is sensitive but has low specificity; thus, false positive results can occur.
- Direct immunofluorescence or immunohistochemistry:
Important Facts
- Suggestive history (multiple chronic skin lesions that may be pruritic and exacerbated by sunlight) and typical clinical signs (multiple annular to polycyclic, hyperpigmented plaques, macules, and papules mostly localized to the head, neck, trunk, and extremities) are important information for a definitive diagnosis.
- Histopathology is essential for a definitive diagnosis and it will show hydropic/vacuolar degeneration of the basal cell layer with individual apoptosis of keratinocytes, with or without lymphocytic satellitosis. These changes can also affect the infundibulum and isthmus of hair follicles.
- Direct immunofluorescence or immunohistochemistry will show deposition of immunoglobulin and/or complement at the dermal-epidermal junction. Remember! False positives and negatives results may occur.
- ANA test has usually low titer or is negative.
-
Treatment
- Based on the few published reports, the prognosis appears to be good with appropriate therapy.
- One or more of the following treatment options can be tried: (See below “Therapy for Autoimmune Diseases” for dose or specifics on treatment regimens).
- Glucocorticoids – Oral and topical.
- Hydroxychloroquine sulfate.
- Cyclosporine.
- 0.1% tacrolimus.
- Oclacitinib – Consider its use for refractory cases as anecdotal reports have shown its efficacy in facial discoid lupus erythematosus and other autoimmune-immune-mediated diseases.
- Doxycycline and niacinamide. Avoid this treatment modality if possible to prevent bacterial resistance to antibiotics (practice antibiotic stewardship).
-
Prognosis
- Clinical signs appear to respond to a wide range of treatments but recurrence was reported in about half of the cases when reduction of drug dose was attempted.
References
Medleau L, Hnilica KA. Chapter 8. Autoimmune and immune-mediated skin disorders. In: Small Animal Dermatology: A color Atlas and Therapeutic Guide 2006. 2nd ed. W.B. Saunders, Missouri, 189-227.
Miller, Griffin and Campbell. Chapter 9. Autoimmune and immune-mediated dermatoses. In: Muller & Kirk’s Small Animal Dermatology 2013. 7th ed., W.B. Saunders, Missouri; 432-462.
Olivry T. Auto-immune skin disease in animals: time to reclassify and review after 40 years. BMC Vet Res 2018; https://doi.org/10.1186/s12917-018-1477-1.
Olivry T, Chan LS. Autoimmune blistering dermatoses in domestic animals. Clin Dermatol 2001; 19(6):750-760.
Olivry T, Linder KE, Banovic F. Cutaneous lupus erythematosus in dogs: a comprehensive review. BMC Vet Res 2018; https://doi.org/10.1186/s12917-018-1446-8.
