2.11 Otitis Media – Dogs and Cats
Learning Objectives
- Know how to diagnose otitis media.
- Remember! Otitis media occurs either from progressing chronic otitis externa (typically in dogs) or from diseases originating in the middle ear or the nasopharynx (typically in cats).
- Know the clinical signs associated with otitis media.
- Remember! In otitis media, the tympanic membrane often appears abnormal or bulging outward; however, a normal appearing and intact tympanic membrane does not rule otitis media.
- Know when to perform myringotomy.
- Remember! Proper treatment should include identifying and resolving or controlling primary diseases and predisposing factors. This is a very important step in helping prevent recurrences. Moreover, performing a thorough lavage of the bulla with sterile saline, under general anesthesia, prior to starting medical therapy increases the chances of success.
- Remember! Selection of antibiotic for the treatment of otitis media should not be extrapolated from cytology and bacterial culture obtained from the external canals, as the organisms are rarely the same. It should be based on culture results of samples collected from the middle ear.
-
General Considerations
- Otitis media is defined as a disease that occurs within the middle ear or tympanic bulla.
- It can be acute or chronic.
- Otitis media may be a primary disease or secondary to chronic otitis externa.
- Otitis media is a common perpetuating factor in cases of chronic otitis externa.
Important Facts
- Otitis media is defined as a disease that occurs within the middle ear or tympanic bulla.
- Otitis media can be acute or chronic and primary or secondary.
- Otitis media is a common perpetuating factor in cases of chronic otitis externa.
-
Etiology and Pathogenesis
- Otitis media can occur as a progression or an extension of chronic otitis externa.
- This is a common cause of otitis media in dogs.
- It can result from (i) infectious diseases originating in the nasopharynx and ascending via the Eustachian tube to the middle ear, (ii) hematogenous spread or (iii) a primary disease originating within the tympanic bulla.
- The most common cause of otitis media in cats appears to be the ascendance of upper respiratory viral or bacterial pathogens to the middle ear via the Eustachian tube.
- Inflammatory polyp in the middle ear can be a cause of primary otitis media in cats.
- The most common cause of otitis media in cats appears to be the ascendance of upper respiratory viral or bacterial pathogens to the middle ear via the Eustachian tube.
- Otitis media can occur as the result of accumulation of fluid or mucous in the middle ear. This condition is named “otitis media with effusion”(OME).
- The cause of OME is unknown at this time. The following may play a role:
- Dysfunction of the Eustachian tube leading to decreased drainage and accumulation of mucous/fluid in the middle ear.
- Increased production of mucous/fluid by the ciliate epithelium lining the middle ear.
- OME is seen more often in brachycephalic breeds such as boxers and Boston terriers.
- Skull conformation in brachycephaly animals can result in obstruction of the Eustachian tube leading to fluid/mucous accumulation in the middle ear.
- Primary secretory otitis media (PSOM) is a well-recognized primary middle ear disease most commonly diagnosed in Cavalier King Charles spaniels. It can be considered a form of OME.
- The cause of OME is unknown at this time. The following may play a role:
- Case reports in cats showed a possible association between the presence of soft palate abnormalities and otitis media probably because the soft palate’s musculature participates in the function of the Eustachian tube.
- Otitis media can occur as a progression or an extension of chronic otitis externa.
Important Facts
- Otitis media can be caused by the following: (i) extension or progression of chronic otitis externa (common in dogs), (ii) ascendance of upper respiratory pathogens to the middle ear via the Eustachian tube (common in cats), (iii) accumulation of mucous/fluid in the middle ear due to increased production or reduced drainage (common in brachycephalic dogs).
-
Clinical Signs
- Otitis media may be unilateral or bilateral.
- Most dogs will have signs of chronic otitis externa because the otitis media is frequently an extension of long-term otitis externa.
- It can be asymptomatic, especially in cats, and be an accidental finding at the time of advanced imaging for other reasons.
- Pain may be present and can be manifested by whining, holding the head to one side, sensitivity when the pinna is gently stretched, reluctance to open the mouth, catch a ball, and chew hard food, yawn or bark.
- Partial or complete hearing loss may be present but it is not a common complaint.
- Head tilt, ataxia and nystagmus may develop if the middle ear disease has extended to the inner ear.
- Sympathetic nerve damage manifested by Horner’s syndrome may develop and is more common in cats. It is characterized by ipsilateral miosis, ptosis, narrowing of the palpebral fissure, enophthalmos, and protrusion of the third eyelid.
- Facial nerve damage may develop and is more common in dogs. It is manifested as ipsilateral ear and lip drooping, widened palpebral fissure, drooling, reduced or loss of corneal, palpebral and menace responses and keratoconjunctivitis sicca if eye lubrication is not instituted.


-
- In the presence of otitis media, an otoscopic exam can reveal an abnormal (i.e. opaque, bulging etc.) but intact tympanic membrane or a ruptured membrane.
- Although otitis media is less likely in the presence of a normal appearing tympanic membrane, this does not rule out otitis media.
- In the presence of otitis media, an otoscopic exam can reveal an abnormal (i.e. opaque, bulging etc.) but intact tympanic membrane or a ruptured membrane.
Important Facts
- Otitis media can be unilateral or bilateral.
- Pain when opening the mouth may be a clinical sign of otitis media.
- Horner’s syndrome is seen more often in cats with otitis media than dogs.
- Facial nerve damage is more common in dogs than cats with otitis media.
- Head tilt, ataxia, and nystagmus may be present if the otitis media had extended to the inner ear.
- The tympanic membrane may appear ruptured, opaque or bulging outward; however, a normal appearing and intact tympanic membrane do not rule out otitis media.
-
Diagnosis
- History and physical examination:
- Otitis media should be suspected in (i) cases of chronic, relapsing, or refractory otitis externa (especially in dogs), (ii) when the tympanum appears abnormal or is ruptured, and/or (iii) when neurologic signs are present.
- A thorough dermatological and neurological history and physical examination are fundamental diagnostic procedures.
- Examine the face for signs of facial nerve paralysis (especially dogs) or Horner’s syndrome (especially cats) and, in advanced cases, signs of inner ear (head tilt, nystagmus, ataxia) involvement.
- Examine the oral cavity for evidence of inflammation and masses in the oropharyngeal area (especially polyps in cats).
- Observe the patient for signs of pain when opening the mouth, which can occur in severe otitis media cases.
- Perform a hand-held otoscopic examination or, if available, a video otoscope examination to evaluate the external ear canal and tympanic membrane.
- Sedation or/and anesthesia may be necessary to perform a thorough otoscopic examination.
- Assessment of the tympanic membrane is a very important diagnostic step. It will help recognize if the tympanic membrane is intact and normal, intact but abnormal, ruptured or if it has healed after an episode of infection.
- The tympanic membrane may appear normal in rare cases of otitis media.
- Abnormalities of the tympanic membrane that may indicate otitis media include: (i) opacity and thickening of the pars tensa with loss of the normal striations; (ii) material such as discharge, debris, and fluid behind an intact tympanic membrane; and (iii) bulging appearance.
- Small tears/rupture of the tympanic membrane may be missed with hand-held otoscopes.
- The patency of the tympanic membrane may be assessed by the following ways:
- Using a hand-held otoscope and filling the canal with warm saline and looking for air bubbles rising as the animal breathes.
- Gentle probing of the tympanum may be performed using a small-diameter catheter — if the probe bounces of a spongy surface, it is likely the tympanum is intact – if it bounces of a hard surface, it is more likely to be hitting the cochlear promontory suggesting rupture of the tympanic membrane.
- Instilling a dye, warm water, warm dilute povidone iodine or dilute fluorescein into the ear canal — if fluid is visualized through the nose or throat it suggests rupture of the tympanic membrane.
- CT scan or MRI.
- Imaging:
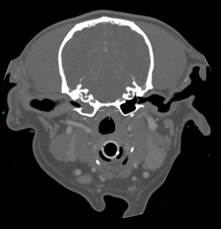
- Radiography, CT scan and MRI are very useful to assess the middle ear and to confirm the diagnosis of otitis media and the presence of polyps or masses.
- Radiography can assist with identification of otitis media and proliferative or lytic changes in the bulla bone in chronic cases. Approximately 25% of otitis media cases in dogs and cats have no radiographic changes. Therefore, normal radiographic findings do not exclude middle ear disease.
- CT scan is very useful in differentiating bony lesions within the bulla from soft tissue lesions. It is better in diagnosing soft tissue changes and otitis media compared to x-rays.
- It is the most common method used to diagnose otitis media in dogs and cats because of its availability, reduced cost, and shorter scanning time compared to MRI.
- History and physical examination:

-
-
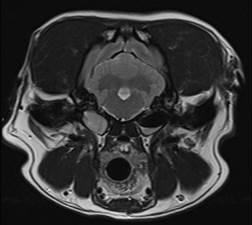
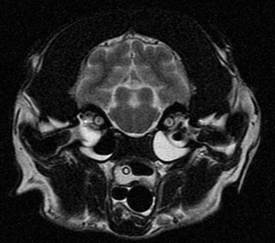
- MRI can also be used to examine the middle ear and identify otitis media, polyps and masses; however, it is more useful in investigating soft tissue and especially inner ear problems, which are less commonly seen in dogs and cats. Bone structures cannot be visually adequately with MRI. It may be cost prohibitive.
-
-
-
- Normal CT scan and MRI findings diminish the chances of the patient having otitis media but do not rule it out.
-
Important Facts
- A thorough dermatological history and physical examination are fundamental diagnostic procedures.
- Assessment of the tympanic membrane is a very important diagnostic step.
- When the tympanic membrane is intact but appears abnormal or when it is ruptured, otitis media should be suspected.
- Despite uncommon, the tympanic membrane can appear normal in the presence of otitis media.
- Advanced imaging, such as CT scan, is a sensitive test to confirm the diagnosis of otitis media and the presence of polyps or masses in the middle ear. However, normal findings do not rule it out.
- MRI is better than CT scan to diagnose soft tissue abnormalities and CT scan is better to diagnose bony abnormalities.
-
- Myringotomy:
- Myringotomy is an incision made in the tympanic membrane to allow access to the middle ear.
- The following are rationales for doing a myringotomy:
- Obtain samples for cytology and microbial culture in cases of confirmed middle ear disease where the tympanic membrane is intact.
- Remove fluid or mucus from the middle ear cavity and reduce the pressure created by accumulation of fluid/mucus.
- Thorough flushing of the middle ear as part of the treatment protocol of otitis media.
- When to consider performing a myringotomy:
- Presence of signs consistent with otitis media associated with an abnormal appearance of the tympanic membrane or an abnormal middle ear on diagnostic imaging.
- Abnormal appearance of an intact tympanic membrane on otoscopic exam.
- Advance imaging showing middle ear disease.
- General anesthesia is required.
- Myringotomy technique:
- It is recommended that advanced imaging (CT scan) be performed before the procedure.
- Myringotomies should be ideally performed with a video otoscope because it is very difficult to evaluate the integrity of the tympanic membrane and perform the procedure with a hand-held otoscope.
- The external ear canal should be thoroughly flushed with warm sterile 0.9% saline to remove debris and discharge. If large amounts of discharge/debris are present, a non-ototoxic ceruminolytic cleaner (e.g. squalene) can be applied in the external canal and allowed to soak for about 10 minutes to more effectively remove the debris and discharge. The ear canal is then flushed with sterile saline.
- Make sure to collect samples for cytology before cleaning the external canal if signs of otitis externa is present.
- After cleaning of the external canal, suction out completely the cleaner and water to reduce the risks of contaminating the middle ear during the myringotomy,
- A sterile polypropylene 5 French urinary catheter cut to about a 30cm length and a 90° tip angle, will be inserted gently through the pars tensa of the tympanic membrane.
- The catheter is placed inside the port and channel on the video otoscope and used to make the incision.
- To avoid damaging the middle ear structures, it is important to insert the catheter at the five or seven o’clock position (i.e. caudal-ventral quadrant).
- After the incision is done, advance the catheter until it touches bone.
- A syringe is attached to the catheter and the fluid gently aspirated back. If the sample is dry, about 1 mL of sterile saline is instilled into the bulla and then aspirated back.
- The fluid obtained from the middle ear should be used for cytological analysis and bacterial culture and susceptibility.
- Thereafter, the middle ear is gently flushed with saline and the fluid aspirated through the incision multiple times to clean and dry the middle ear as thoroughly as possible.
- An aqueous antibiotic solution can be applied directly into the middle ear right after the flush, if bacteria is seen on cytology. Drugs known to be ototoxic should be avoided (see below under “Treatment”).
- An aqueous glucocorticoids solution, such as dexamethasone sodium sulfate (4mg/ml), can also be applied directly into the middle ear immediately after the flushing.
- Myringotomy complications are uncommon and tend to occur more commonly in cats than dogs.
- These include head tilt, Horner’s syndrome (enophthalmos, ptosis, miosis, and protrusion of the nictitating membrane), vestibular symptoms (head tilt, ataxia, and circling) and deafness.
- In most cases, once the otitis media is resolved, the tympanic membrane will heal within 3-6 weeks.
- Myringotomy:
Important Facts
- Myringotomy is useful to collect samples from the middle ear in cases of confirmed or suspected otitis media for cytology and culture and to remove and flush fluid and mucus.
- Myringotomy requires general anesthesia and ideally should be performed by an experienced clinician with the use of a video-otoscope.
-
Cytology and Culture
- Cytological analysis and bacterial culture and susceptibility from samples obtained from the middle ear should be performed in all cases of otitis media.
- Care should be taken to avoid microbial contamination of the middle ear with material from the external ear canal during flushing and myringotomy.
- Cytological examination of swab specimens was not as effective for detection of rods and cocci from the middle ear when compared with results of bacterial culture; therefore, culture is very important in cases of otitis media to completely rule out a bacterial infection.
- Cytological analysis and bacterial culture and susceptibility from samples obtained from the middle ear should be performed in all cases of otitis media.
-
Treatment
- Because otitis media can be the result of extension of chronic otitis externa through a ruptured tympanic membrane, all the principles discussed for otitis externa apply here.
- Successful treatment also means identifying and resolving or controlling primary diseases and predisposing factors.
- In Hospital Otic Flush:
- A thorough lavage of the bulla with sterile saline, under general anesthesia, to remove infective and inflammatory exudate will be very important prior to starting medical therapy. Medical failure is very likely without a thorough flush of the middle ear.
- A non-ototoxic aqueous solution of antibiotic combined with an aqueous solution of a glucocorticoid (e.g. dexamethasone sodium sulfate (4mg/mL) can be applied directly in the middle ear and immediately after the flush, when the patient is still anesthetized.
- Products reported to be non-ototoxic: Aqueous dexamethasone, aqueous fluocinolone, ciprofloxacin, enrofloxacin, ofloxacin, penicillin G, carbenicillin, ticarcillin (controversial), ceftazidime, cefmenoxine, miconazole, clotrimazole, nystatin, tonalftate, squalene, triz-EDTA
- Products reported to be ototoxic: Organic acids (salicylic, malic and lactic), detergents and alcohols, chlorhexidine, gentamicin, amikacin, tobramycin, neomycin, polymyxin B and most ceruminolytics.
- Veterinarians performing otic lavage must have experience with the procedure to minimize complications. Additionally, the lavage of the bulla is best accomplished by using a video-otoscope.
- Potential complications associated with otic flushing should be discussed with the owners prior to the procedure. Complications from ear flushing are infrequent in dogs but more common in cats (see above).
- Fortunately, most otic flush complications are transient, but owners should be aware that permanent neurologic damage is possible. Possible complications include:
- Pain and head shaking,
- Horner’s syndrome (enophthalmos, ptosis, miosis, and protrusion of the nictitating membrane) or facial nerve injury (drooped lip and ear, inability to close the eyelid, and decreased palpebral reflex).
- Vestibular symptoms (head tilt, imbalance, and circling) and deafness.
- It is important to be gentle and patient during the middle ear flushing procedure.
- Ear flushes may need to be repeated for a more favorable outcome.
- Because the therapeutic benefits of this procedure exceed its risks, veterinarians should always recommend otic flushing for patients with suspected or confirmed otitis media.
- There is no completely safe solution for cleaning the middle ear and sterile saline is most frequently used.
- If imaging studies are to be performed at the same day as the flush procedure, they should precede the placement of any fluids into the ear.
- Outpatient Medical therapy:
- Antimicrobials and glucocorticoids that are likely to not be ototoxic may be instilled in the bulla right after the flushing, to help treat infections and minimize inflammation and discomfort associated with the procedure, respectively.
- Otitis media should not be treated with topical therapy alone because medications applied in the external ear canal may not reach the middle ear effective.
- Topical and systemic antibiotic therapy should be selected based on cytological analysis and bacterial culture and susceptibility.
- Selection of antibiotics for the treatment of otitis media should not be extrapolated from cytology and bacterial culture obtained from the external canal, as the organisms are rarely the same. One study showed that a difference in total isolates or susceptibility patterns between the horizontal ear canal and middle ear was found in 34 (89.5%) ears.
- Systemic antibiotic therapy for the treatment of otitis media should be administered for at least 6-8 weeks even if the clinical signs (when present) resolve sooner.
- Ideally, duration of therapy should be guided by the results of imaging, cytology and bacterial culture of the middle ear. However, because these tests require general anesthesia and are costly to the pet owner, unfortunately they are not performed in most cases.
- Topical and/or systemic glucocorticoids are often beneficial to help reduce otic inflammation and discharge and minimize discomfort after the flushing procedure.
- Regular cleaning at home, in addition to targeted antimicrobial therapy should be used for a minimum of 6 to 8 weeks.
- In cases of polyps or tumors, surgical excision is recommended.
Note: Refer to “Otitis Externa” for details on antibiotic, antifungal and ear cleaners, in addition to ototoxicity and surgical therapeutic options.
Important Facts
- Proper treatment means identifying and resolving or controlling primary diseases and predisposing factors. In addition, performing a thorough lavage of the bulla with sterile saline, under general anesthesia, prior to starting medical therapy is an important part of the treatment regimen.
- Otitis media should not be treated with topical therapy alone.
- Topical and systemic antibiotic for the treatment of otitis media should be selected based on cytology and bacterial culture and susceptibility results of samples collected from the middle ear, not the external canal.
- Regular cleaning at home, in addition to targeted systemic antibiotic therapy should be used for a minimum of 6 to 8 weeks.
References
Belmudes A, Pressanti C, Barthez PY et al. Computed tomographic findings in 205 dogs with clinical signs compatible with middle ear disease: a retrospective study. Vet Dermatol 2017; DOI: 10.1111/vde.12503.
Bishoff MG, Kneller SK. Diagnostic imaging of the feline and canine ear. Vet Clin North Am: Small Anim Pract 2004; 34(2): 437-558.
Brame B, Cain C. Chronic otitis in cats: Clinical management of primary, predisposing and perpetuating factors. J Feline Med Surg 2021; 23: 433-446.
Garosi LS, Lowrie ML, Swinbourne NF. Neurological manifestations of ear disease in dogs and cats. Vet Clin Small Anim 2012; 42: 1143-1160.
Gortel K. Otic flushing. Vet Clin North Am: Small Anim Pract 2004; 34(2): 557-565.
Greci V, Mortellaro CM. Management of otic, nasopharyngeal, and nasal polyps in cats and dogs. Vet Clin Small Anim 2016; 46: 643-661.
Griffin GE, Kwochka KW & Macdonald JM. Diseases of the Ear. In: Current Veterinary Dermatology: The Science and Art of Therapy. Mosby Year Book, St Louis, 1993, p 245-262.
Jacobson L, Janke KJ, Kennedy SK, et al. A Pandora’s box in feline medicine: presenting signs and surgical outcomes in 58 previously hoarded cats with chronic otitis media-interna. J Feline Med Surg 2023; doi/10.1177/1098612X231197089.
Koch SN, Torres SMF, Plumb DC. Canine and Feline Dermatology Drug Handbook Small 2012. Wiley-Blackwell, Ames, Iowa. p. 369-393.
Mansfield PD, Steiss JE, Boosinger TR et al. The effect of four commercial ceruminolytic agents on the middle ear. J Am Anim Hosp Assoc 1997; 33:479-486.
Morris DO. Medical therapy of otitis externa and otitis media. Vet Clin North Am: Small Anim Pract 2004; 34(2): 541-555.
Woodbridge NT, Baines EA, Baines SJ. Otitis media in five cats associated with soft palate abnormalities. Vet Rec 2012; 171: 124.
