3.24 Cutaneous Onchocerciasis – Equine
Learning Objectives
- Learn what causes equine Onchocerca dermatitis.
- Considering that many horses are infected with the microfilariae why do some animals develop a dermatitis?
- Learn the three cutaneous syndromes probably related to Onchocerca cervicalis microfilariae.
- Know the lesion most suggestive of onchocerciasis.
- Learn the most common causes of ventral midline dermatitis in horses.
- Learn how to diagnose onchocerciasis.
- Learn how to treat onchocerciasis.
-
General Considerations
- Onchocerca cervicalis is a filarid nematode parasite of horses.
- The adult nematode resides in the ligamentum nuchae and produces microfilaria.
- The microfilariae migrate via the connective tissue (not the blood) to the upper layers of the dermis.
- Around 95% of the microfilariae locate in the skin of the ventral midline, face, and eyelids.
- The microfilariae are ingested by the vector, Culicoides spp., feeding on the ventral surface of infected horses.
- A high percentage of horses in most parts of the Southern U.S. are infected and the vast majority have no clinical problems.
- However, some horses will develop an inflammatory skin reaction to the Onchocerca cervicalis microfilariae. This disease is known as onchocerciasis.
-
Cause and Pathogenesis
- Most dermatitis localized to the ventrum attributed to Onchocerca cervicalis microfilariae in the past are likely the result of Culicoides spp. and/or horn fly bites.
- As with many filarid infections, great care must be taken to separate the pathology resulting from the microfilariae from the pathology resulting from the effects of the vector.
- The simple presence of large numbers of microfilariae in the skin will not necessarily produce disease.
- The death of the microfilariae may be involved in the pathogenesis.
- A hypersensitivity reaction to the microfilariae may occur, resulting in ocular and dermatologic inflammatory lesions.
-
Clinical Signs
- Three cutaneous syndromes that may be related to Onchocerca cervicalis microfilariae include:
- Inflammatory lesions involving the face and periorbital region.
- The lesions can be diffuse or patchy and consist of alopecia, scaling, and depigmentation.
- Some horses have lesions limited to the depigmented areas of the face resembling photosensitization.
- Bull’s eye lesion in the center of the forehead is suggestive of the disease.
- Diffuse inflammatory disease involving most of the ventral body surface.
- This syndrome is probably related to the vector (Culicoides spp.) and not the microfilariae.
- Inflammatory lesions involving the face and periorbital region.
- Three cutaneous syndromes that may be related to Onchocerca cervicalis microfilariae include:

-
-
- Focal to diffuse crusting, alopecia and depigmentation of the skin at the base of the mane and/or anterior-medial aspect of the forelegs up by the brisket.
-

-
- In general, the disease is nonseasonal and mildly pruritic; however, some believe that the disease is seasonal and moderately pruritic.
- There is a potential for scarring of the affected areas and, therefore, for lack of hair regrowth.
- Remember! Focal, seasonal, and inflammatory lesions on the ventral midline of horses referred to as “ventral midline dermatitis” are probably related to the bites of Culicoides spp. and/or the bites of horn flies and not due to the Onchocerca cervicalis microfilariae.
-
Diagnosis
- Differential diagnoses include dermatophytosis, dermatophilosis, photosensitization, insect bite hypersensitivity, and ventral midline dermatitis.
- Since a high percentage of horses are infected with the nematode, the simple demonstration of microfilariae in diseased skin is not enough to infer a cause and effect relationship.
- The most likely candidates are those horses with nonseasonal facial dermatitis.
- Every attempt should be made to rule out other causes for the skin disease.
- The following technique can be used to demonstrate microfilariae:
- A small piece of skin is removed from the affected area and minced with a scalpel blade, placed on a glass slide, covered with a few drops of physiologic saline solution, and allowed to incubate at room temperature for 5 to 10 minutes or longer if necessary.
- Live microfilariae can be seen easily because of their vigorous movement in the saline solution.
- Ventral midline skin should be avoided.
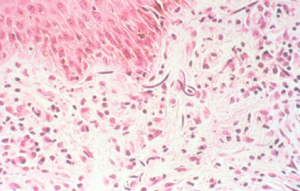
- Histopathology should reveal purple stained microfilariae surrounded by an inflammatory reaction of predominantly eosinophils and lymphocytes.
-
- Response to ivermectin therapy is a practical diagnostic method. Eight weeks should be allowed for the response.
-
Treatment
- Ivermectin given orally at a dosage of 200 µg/kg. One dose is sufficient.
- Response to ivermectin therapy will differentiate onchocerciasis from insect bite hypersensitivity or insect bite reaction.
- Response to therapy should be seen in 8 weeks.
- Some horses will develop facial and/or abdominal edema after this treatment. This is presumed to be an allergic reaction elicited by the death of the microfilariae but it occurs less frequently with ivermectin than with diethylcarbamazine (DEC) or levamisole. Presumably, ivermectin kills the microfilaria more slowly.
- An ophthalmic exam should be made prior to therapy because death of microfilariae will exacerbate a pre-existent uveitis. Eyes should be pretreated with steroids.
- Systemic corticosteroids may be given for the first 3 or 4 days of therapy; 400 to 500 mg of prednisolone per horse is the usual dose.
- Clinical response may be noted as early as day 3 or 4 of therapy and most horses have shown good response in 2 to 3 weeks.
- Since the adult nematodes are not killed, retreatment will usually be required in 2 to 12 months when the skin has become repopulated with microfilariae.
- Treat early if possible. Considerable scarring with destruction of hair follicles can occur in chronic cases.
Important Facts
- Equine cutaneous onchocerciasis is a dermatitis caused by the microfilariae of the nematode Onchocerca cervicalis, which lives in the ligamentum nuchae of most horses.
- Most horses are infected with the nematode but only a small percentage will develop a dermatitis induced by the microfilaria.
- As a result, the simple demonstration of the microfilaria in the skin does not necessarily indicate that the parasite is causing the presenting dermatitis.
- Most cases of dermatitis localized to the ventral midline are caused by bites of the nematode vector Culicoides spp. and/or bites of the horn fly.
- Alopecia, scaling, crusts, and depigmentation of the skin are usually present on the face, periorbital region, ventral midline, base of the mane and forelegs.
- Nonseasonal cases with a bull’s eye lesion in the center of the forehead are more likely to have cutaneous onchocerciasis.
- The most practical diagnostic method is response to ivermectin therapy.
- Response to this treatment trial will differentiate onchocerciasis from insect bite lesions or insect bite hypersensitivity.
- Ivermectin is the current treatment of choice and one dose is sufficient.
- Since ivermectin does not kill the adult worms, retreatment is usually necessary in 2 to 12 months.
References
Fadok VA, Mullowney PC. Dermatologic diseases of horses Part I. Parasitic dermatoses of the horse. Compend Cont Educ 1983; 5: 615-622.
Efficacy of ivermectin in paste and injectable formulations against microfilariae of Onchocerca cervicalis and resolution of associated dermatitis in horses. Am J Vet Res 1988; 49: 1550-1554.
Lees MJ, Kleider N, Tuddenham TJ. Cutaneous onchocerciasis in the horse: five cases in southwestern british columbia. Can Vet J 1983; 24: 3-5.
Onchocerca cervicalis in horses: dermal histopathology. Acta Trop 1985; 42: 55-61.
Scott DW. Parasitic Diseases. In: Large Animal Dermatology. 1st ed. Philadelphia, PA: W.B. Saunders, 1988; 266-267.
